




Abstract
Wrinkles are just one indicator of facial aging, but an indicator that is of prime importance in our world of facial aesthetics. Wrinkles occur where fault lines develop in aging skin. Those fault lines may be due to skin distortion resulting from facial expression or may be due to skin distortion from mechanical compression during sleep. Expression wrinkles and sleep wrinkles differ in etiology, location, and anatomical pattern. Compression, shear, and stress forces act on the face in lateral or prone sleep positions. We review the literature relating to the development of wrinkles and the biomechanical changes that occur in response to intrinsic and extrinsic influences. We explore the possibility that compression during sleep not only results in wrinkles but may also contribute to facial skin expansion.
Wrinkles are inevitable and while a few lines may be endearing, most of us would prefer to keep them in check. When we consider wrinkles we generally think of the lines of facial expression. While facial animation is responsible for the most significant wrinkle patterns, not all wrinkles of the face are due to muscle contraction. Sleep wrinkles develop in response to distortion created when the face is pressed against any sleep surface. Compression, shear, and stress forces result in facial distortion in side or stomach sleeping positions. In contrast, the only external forces acting on the face in the supine position are gravitational.
Wrinkles can become permanent with time and repetition. In a young face, wrinkling is transient with animation and sleep wrinkles disappear on awakening. The rate and severity of wrinkling varies as skin ages in response to intrinsic and extrinsic influences combined with repetition of force patterns.
Sleep wrinkles differ from expression wrinkles in mechanism of origin (external forces vs internal muscle contraction), location (wrinkles likely occur at the limits of retaining ligaments vs site of muscle contraction), and directionality (mostly perpendicular to each other). We suggest these are sufficient reasons to reconsider wrinkle classification and consider the possibility that facial distortion during sleep not only results in sleep wrinkles, but may also contribute to overall facial aging.
Why do wrinkles occur? Wrinkles are only one component of a complex series of changes that occur as we age. Intrinsic and extrinsic factors determine biochemical and cellular aging changes and these, in turn, determine the biomechanical properties and ability of skin to respond to internal and external forces.
Wrinkle Classification
Wrinkle scales exist that are oriented toward treatment or grading of wrinkles for comparisons.1 Various wrinkle classification systems have been proposed to categorize based on differences in wrinkle histology and mechanism of development.2-5 To date, sleep wrinkles have not been recognized in any classification system.
Pierard recognized 4 categories based on histological differences and suggested causes:6-8
Atrophic wrinkles develop in exposed and non-exposed skin, disappear with skin traction, change in orientation with body posture, and are due to atrophy of the extracellular matrix.
Elastotic wrinkles develop in sun exposed skin, exhibit solar elastosis, become progressively permanent, and do not disappear with perpendicular traction.
Expressional wrinkles due to subdermal muscle contraction, become permanent with repeated wrinkling.
Gravitational wrinkles due to skin sagging in response to gravitational forces and inelasticity.
Pierard's “gravitational wrinkles” result from the impact of external forces due to Earth's gravity. Compression, tension, and shear forces applied to the face during sleep may have an even greater impact on wrinkle development than gravity alone.
Histology of Aging Skin
Sun exposure (ultraviolet and infrared radiation), smoking, and other extrinsic, environmental factors combine with intrinsic aging signals (chronologic age, hormonal status) to produce typical histologic features of aging skin.9 The most consistent feature of skin aging is stiffening of the stratum corneum and dermis.10-14 Changes in dermal collagen, elastin fiber quality, proteoglycans, and water content all contribute to stiffening of the dermis with age.4 The more superficial epidermis stiffens with age due to drying of the stratum corneum.10 Increased dermal and epidermal stiffness are important factors in the changes in biomechanical properties demonstrated with age.
Reported changes in skin thickness vary considerably. Total skin thickness is increased in sun exposed sites (except orbital skin) and may decrease with intrinsic aging alone.12,15,16 Overall, the dermis either thins or remains unchanged except for the Sub-Epidermal Non-Echogenic Band (SENEB) which characteristically increases in thickness with UV exposure. The epidermis is either decreased or unchanged with age.10,15,17,18 The dermoepidermal junction flattens with fewer and decreased amplitude of papillae.10,19
Biomechanics of Aging Skin
As skin ages and stiffens, it's response to applied external forces also changes. We can consider skin as an elastic tissue that deforms in response to external loads including compression, tension, and shear forces. Applied forces result in deformation or strain, and are dependent on the skin's elasticity, stiffness, resilience, and extensibility. These characteristics are dynamic and can vary in the short term and with age.
Elasticity is the ability to recover (recoil) after extension (stretch) and decreases with age. Extensibility and distensibility both refer to skin's resistance to stretch and also decrease with age.10,13,20-23 The ability to return to its initial position after extension decreases with repeated cycles. As expected, this skin fatigue increases with age,23,24
Human skin is also under constant internal tension, accounting for Langer's lines. They represent the direction of maximum skin tension at any site. Necessary for growth, young skin is isotropic, more random in directionality, with multi-directional furrows seen on microrelief. Older skin becomes anisotropic, more uniform in directionality, and represents the direction of maximum tension. Fibroblasts and collagen fibers orient based on, and parallel to, the direction of tension.18,19,25-27 Ultimate directionality is then dependent on the predominant direction of external and internal forces for each skin area.
Wrinkle Formation
Compression of young, elastic skin results in many, thin wrinkles whereas older, less elastic skin results in fewer, wider wrinkles. In elastic skin, reaction to an externally applied force will diminish gradually over a large area whereas the response of inelastic skin will be more localized and decay abruptly over a smaller area.10,28,29
Decreased elasticity (recoil) and decreased extensibility (stretch) are both associated with increased wrinkle formation and both occur with age.21,28,30 Wrinkles seem to occur when a tipping point is reached in the mechanical balance between skin layers. It has been suggested that epidermal and dermal stiffening occur at different rates and the layers successively buckle with compression.11,12,31 Repetitive damage ultimately results in permanent wrinkles and smaller compressive forces generate wrinkles parallel to the direction of skin movement.31-33
Leveque examined silicone replicas of crows-feet 21 years apart.34 Compared to early more isotropic (multi-directional) microrelief, he found the number of wrinkles decreased with age but increased in length and depth in chronically deformed skin. This is consistent with increased anisotropy (uni-directionality) in response to persistent stress.
As expected, the site of temporary wrinkles created with expression predicts the site of permanent wrinkles. More interesting, the severity of temporary wrinkles predicts a faster rate of permanent wrinkle development.34,35 In an 8 year longitudinal study, the combination of mechanical stress and degree of skin inelasticity were important determinants of both age of onset and rate of permanent wrinkling.35,36 The rate of wrinkle formation was highest in women who were in their 40s and in early menopause compared to those who were in their teens or 60s at baseline. Menopausal state, dryness of the skin, and surface pH, even controlling for age correlated with rate of wrinkling.
While the mechanism for expression wrinkle development seems clear, the importance of facial distortion during sleep needs further consideration. Distortion can result in wrinkles, but can it also impact facial aging by skin expansion? There are possible models for external facial distortion causing not only sleep wrinkles, but also contributing to further biomechanical changes.
Tissue expansion is an example of skin “stretch” and slowly increasing expander volume results in short term and permanent changes, especially in the dermis.37,38 Rapid intraoperative tissue expansion has similar effect. Although it requires very high applied forces, external tissue expansion does not require undermining so may offer a model closer to sleep distortion.39
We now know that external (and internal) mechanical forces can signal biochemical changes in the skin. This mechano-chemical transduction network allows remodeling of epidermal, dermal and matrix components.40-42
Transduction of mechanical signals may have broader relevance. Turlier37 has suggested that injection of hyaluronic acid results in dermal and subdermal stretch. This strain change may then activate signaling pathways that result, in this case, to neocollagenesis. Similarly, Botulinum neurotoxin A may have a long-term effect on skin biomechanical properties contributing to improved skin elasticity beyond the duration of obvious muscle weakness.22
Sleep Wrinkles
The concept of sleep wrinkles is not new.43-45 Fulton et al postulated that sleep wrinkles develop due to sleep position and site of SMAS condensation.43 They described the most common sites that sleep wrinkles develop. Polisak attempted to show sleep wrinkles in situ using a transparent polyvinyl chloride (PVC) pillow.45
During side or stomach sleeping, facial tissue is subject to shear, compression, and tensile mechanical forces (Figure 1). The skin is stretched and pulled in all directions with changes in sleep position. These forces become significant when we consider the amount of time spent in sleep and sleep position.
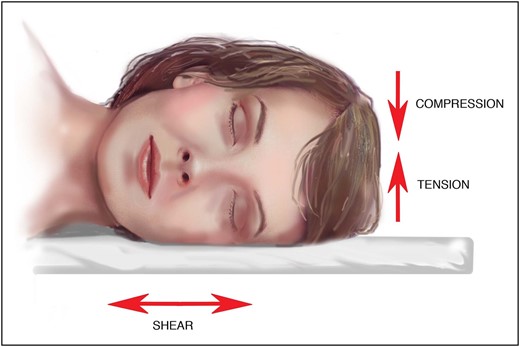
External forces (including compression, tension, and shear) act on facial tissue in lateral or prone sleep positions.
During sleep, the spinal column unloads, intervertebral discs rehydrate, discs regain elasticity, and peri-spinal muscles relax.46,47 While our initial sleep position is a conscious decision, we change positions throughout the night as our bodies unconsciously attempt to minimize ischemia and discomfort.47,48 With age, the number of position shifts decrease from 27 to 16 per night, with an average of 20 position shifts per night.47-50 Consequently, the time spent in each position increases with age. The lateral sleep position is most common in all studies averaging 65% lateral, 30% supine, and 5% prone.47,48,50 It is uncommon for an individual to spend 100% of their sleep time in a single sleep position.
Wrinkles of facial expression begin as many, small, superficial creases perpendicular to the axis of muscle contraction and parallel to the axis of skin compression. As skin loses elasticity and stiffens, they progress to fewer, deeper creases which become permanent with repetition and age. We expect the same process to occur regardless of the source of force. The rate of onset and severity would similarly vary with genetics, sun exposure, smoking, and hormonal status.
Lines of facial expression (Figure 2A) are commonly recognizable and easily confirmed by replication with animation. Careful examination of the face, however, reveals other wrinkles that cannot be reproduced with animation (Figure 2B). These sleep lines are easily reproducible with a hand, by imitating compression caused by sleep. They tend to be perpendicular to expression lines. We have identified the most common sleep wrinkles (Figure 3).
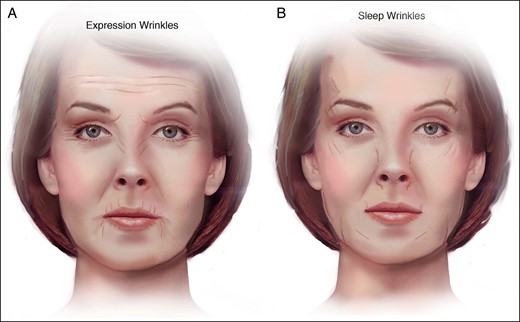
(A) Common expression wrinkles. (B) Common sleep wrinkles.
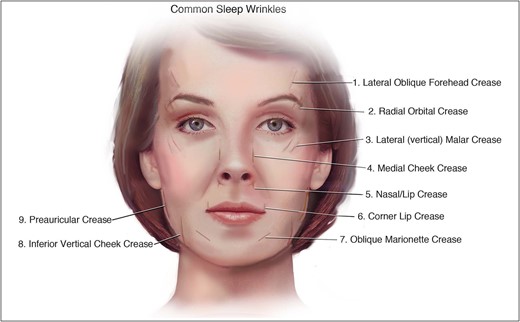
Sleep wrinkle sites identified.
Figures 4 and 5 identify multiple sleep wrinkle sites in a single patient. The cause of the proposed sleep wrinkles can be demonstrated with maneuvers to simulate compressive forces (Figures 5 and 6). Animation does not significantly reproduce sleep wrinkles as seen in Figures 4 and 7.
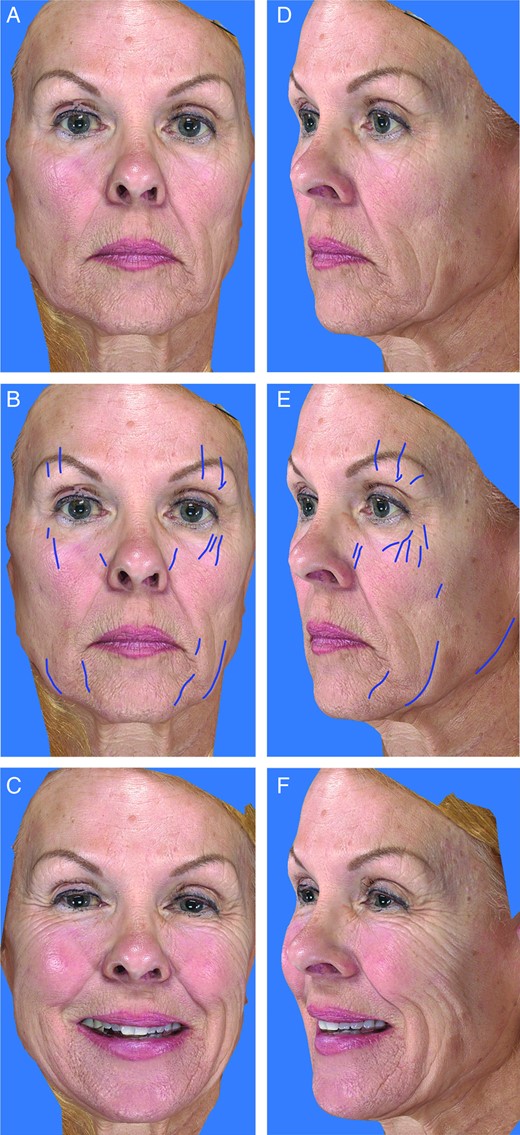
Sleep wrinkles can be distinguished from wrinkles of facial expression. (A, D) A 65-year-old women in repose, (B, E) with sleep wrinkles highlighted, and (C, F) in animation. Images taken with the Vectra 3D Image System (Canfield Scientific, Fairfield, NJ).

(A) Frontal and (B) oblique views on a 58-year-old woman, (C) with sleep wrinkles highlighted, (D) and lateral sleep simulation demonstrating sleep wrinkle etiology.
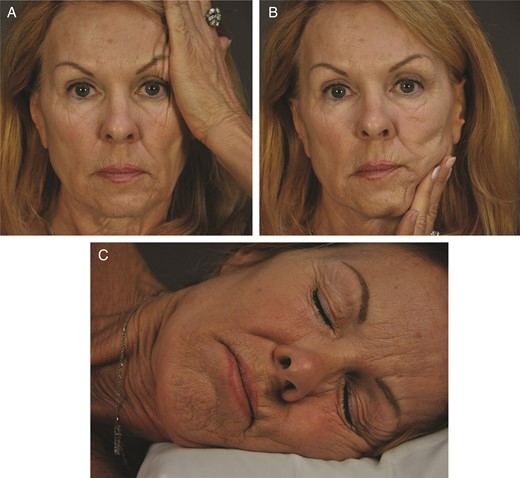
(A, B) Recreation of distortion with hand compression and (C) simulation of lateral sleep posture demonstrates causal forces in this 65-year-old woman.

(A-D) Expression does not significantly reproduce sleep wrinkles in this 65-year-old woman.
The development of sleep wrinkles appears less predictable than expression wrinkles. This is expected if we consider the greater number of variables that influence sleep wrinkle development. First, the age of onset, rate of development, and severity of any wrinkle type shows a wide range among a given population. Susceptibility to wrinkling is dependent on genetics, age, hormonal status, and environmental exposure. Sleep wrinkle pattern will be additionally influenced by how much time is spent in various positions, how much force is applied to each area of the face, and surface area of contact. Expression wrinkles have little variation in the direction of applied forces.
The system of retaining ligaments of the face have been described by Furnas, Mendelson, Pessa, and others.51-56 Sleep wrinkles seem to occur at sites where the skin buckles in response to external forces applied (Videos 1 and 2, available as Supplementary Material at www.aestheticsurgeryjournal.com). The greatest impact of the forces are expected to be in the areas where skin is most tethered to underlying attachments, where retaining ligaments of the face anchor skin to underlying bone (Figure 8). The overlying skin can be thought of as seaweed that sways while tethered to a stalk or retaining ligament. A wrinkle would be expected to occur along the periphery of the mobile skin segment. Indeed, sleep wrinkles are mostly seen at the expected sites associated with retaining ligaments. Only the central medial sleep wrinkles are not associated with a true retaining ligament. These include the medial cheek crease at the nasal/cheek junction, nasal lip crease, and corner lip crease.
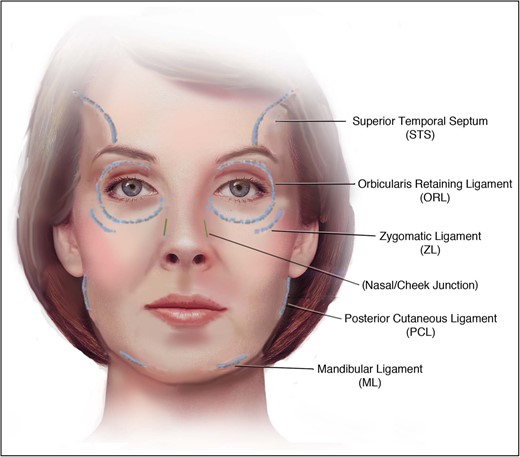
Retaining ligaments of the face are consistent with the location of most sleep wrinkles.
Sleep patterns can also reinforce expression lines. Skin will buckle along weak areas or faults in the superficial skin layers.3,32 We have observed reinforcement of upper lip radial expression lines due to sleep position. Although a wrinkle may initially be caused by muscle contraction, the wrinkle appears to worsen due to compression as seen in Figures 7D and 9A. The presence of a crease from any cause provides an additional fault line that may be preferentially followed. Kotlus did not find an association between sleep side and wrinkles.57 However, they looked at all wrinkles and did not differentiate wrinkle types. They also relied on subjective questionnaires to determine sleep position which is much more variable than subjects estimate.
DISCUSSION
Wrinkles of facial expression are the most important type of facial wrinkle and occupy much of the dermatologist's and plastic surgeon's time outside the operating room. However, review of the literature on facial wrinkles supports recognition of sleep wrinkles as distinct from expression wrinkles with a different etiology. Sleep wrinkles could be grouped with gravitational wrinkles in existing wrinkle classification systems. Conceptually, they both develop in response to external forces and are influenced by ligamentous attachments. Few individuals sleep entirely on their back without some component of non-gravitational forces acting during sleep. The interplay between sleep forces, internal forces and aging changes are more complex than gravitational effects alone.
Facial distortion in sleep contributes to the appearance of aging with the development of sleep wrinkles which alone affect aesthetic appearance. An even greater contribution to aging may be due to the effects of sleep distortion on the bioelastic properties of skin. We postulate a mechanism where skin distortion can act as external skin expansion. Sleep distortion itself may result in progressive increases in maximum extension and residual deformation. Both can occur due to creep (further extension over time with a constant load), or in response to cyclic repetition. Some skin expansion seems likely, and combined with volume loss and other aging factors may contribute to the appearance of aging. Further study is warranted to evaluate the importance of distortion on skin aging.
CONCLUSION
Treatment options for sleep wrinkles and improvement in distortion are more limited than those for expression wrinkles. Facelift and other tightening procedures will decrease the amount of skin available to buckle and possibly alter skin attachments. Fillers can temporarily improve wrinkles of any type. Mechanical stress contributes to the progression of temporary to permanent expression lines. Neurotoxin use improves or prevents wrinkles by eliminating mechanical stress. However, neurotoxins should have no effect on true sleep wrinkles since they are not caused by muscle contraction. The only reliable way to minimize sleep wrinkles is to avoid facial distortion.
While we recommend back sleeping, it is extremely difficult to consciously change sleep patterns. Our initial sleep position is a choice, however we unconsciously change position throughout the night. The supine position may be ideal for facial aesthetics but can aggravate conditions including sleep apnea, gastroesophageal reflux, and severe snoring. Specialty pillows now exist that are designed to minimize facial deformation during sleep (Figure 9). It can take up to 4 weeks to accommodate to a change in bedding system.47,49,58

A 59-year-old woman demonstrating sleep wrinkles reinforced in (A) lateral sleep position and (B) compression reduced with a specialty JuveRest pillow (Las Vegas, NV).
As plastic surgeons, we advise our patients to control the variables that influence aging based on current understanding. We advise our patients use sunscreen to minimize photoaging, quit smoking, optimize nutrition, and maximize topical skin care. We should add avoidance of facial compression during sleep to that list. While avoiding the development of sleep wrinkles may be important, it is the facial distortion and its' potential impact on overall facial aging that may be even more important. The consequence of repetitive stretching of facial tissue over time is intriguing and warrants further study.
Disclosures
Dr Anson is a Partner, JuveRest, LLC (Las Vegas, NV); and Honorarium Recipient and on the Advisory Board, Allergan (Parsippany, NJ). Dr Kane is a Consultant, Stockholder, and Honorarium Recipient, and on the Advisory Board and Speaker Bureau, Allergan; is a Consultant and on the Advisory Board, Mentor/Johnson & Johnson (Santa Barbara, CA); is a Consultant, Honorarium Recipient, and Investigator, and on the Advisory Board and Speaker Bureau, Galderma (Lausanne, Switzerland); is on the Advisory Board, Stiefel (Brentford, UK); is a Consultant, Investigator, and Stockholder, and on the Advisory Board and Speaker Bureau, Revance (Newark, CA); is a Consultant for Shire (Dublin, Ireland), Canfield (Fairfield, NJ), Beiersdorf (Hamberg, Germany), Hancock Jaffe (Irvine, CA), Valeant (Laval, Quebec), Alphaeon (Irvine, CA), L′Oreal (Clichy, France), Premier Pharm (Bangkruay, Thailand), and the Musculoskeletal Transplant Foundation (Edison, NJ); is a Consultant and Investigator, and on the Advisory Board and Speaker Bureau, Merz, (Frankfurt am Main, Germany); is a Consultant and Investigator, Teoxane (Geneva, Switzerland); is a Consultant, Investigator, and on the Advisory Board, Kythera (Westlake Village, CA) and Neothetics (San Diego, CA); and is the Founder, HLA Technologies (New York, NY). Dr Lambros has no disclosures.
Supplementary Material
This article contains supplementary material located online at www.aestheticsurgeryjournal.com.
Funding
The authors received no financial support for the research, authorship, and publication of this article.
REFERENCES


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}