



Abstract
The non-fluent/agrammatic variant of primary progressive aphasia (nfvPPA) presents with a gradual decline in grammar and motor speech resulting from selective degeneration of speech-language regions in the brain. There has been considerable progress in identifying treatment approaches to remediate language deficits in other primary progressive aphasia variants; however, interventions for the core deficits in nfvPPA have yet to be systematically investigated. Further, the neural mechanisms that support behavioural restitution in the context of neurodegeneration are not well understood. We examined the immediate and long-term benefits of video implemented script training for aphasia (VISTA) in 10 individuals with nfvPPA. The treatment approach involved repeated rehearsal of individualized scripts via structured treatment with a clinician as well as intensive home practice with an audiovisual model using ‘speech entrainment’. We evaluated accuracy of script production as well as overall intelligibility and grammaticality for trained and untrained scripts. These measures and standardized test scores were collected at post-treatment and 3-, 6-, and 12-month follow-up visits. Treatment resulted in significant improvement in production of correct, intelligible scripted words for trained topics, a reduction in grammatical errors for trained topics, and an overall increase in intelligibility for trained as well as untrained topics at post-treatment. Follow-up testing revealed maintenance of gains for trained scripts up to 1 year post-treatment on the primary outcome measure. Performance on untrained scripts and standardized tests remained relatively stable during the follow-up period, indicating that treatment helped to stabilize speech and language despite disease progression. To identify neural predictors of responsiveness to intervention, we examined treatment effect sizes relative to grey matter volumes in regions of interest derived from a previously identified speech production network. Regions of significant atrophy within this network included bilateral inferior frontal cortices and supplementary motor area as well as left striatum. Volumes in a left middle/inferior temporal region of interest were significantly correlated with the magnitude of treatment effects. This region, which was relatively spared anatomically in nfvPPA patients, has been implicated in syntactic production as well as visuo-motor facilitation of speech. This is the first group study to document the benefits of behavioural intervention that targets both linguistic and motoric deficits in nfvPPA. Findings indicate that behavioural intervention may result in lasting and generalized improvement of communicative function in individuals with neurodegenerative disease and that the integrity of spared regions within the speech-language network may be an important predictor of treatment response.
Introduction
Primary progressive aphasia (PPA) is a debilitating disorder in which speech and language deteriorate as a result of neurodegenerative disease. Communication difficulty is the earliest and most pronounced symptom, reflecting selective degradation of brain regions important for speech and/or language (Mesulam, 2001; Gorno-Tempini et al., 2011). PPA is increasingly viewed as a disorder of network-based degeneration (Seeley et al., 2009) in which epicentres of brain atrophy are located in critical nodes of the language network (Mandelli et al., 2016). Three clinical variants—non-fluent/agrammatic, semantic and logopenic—are recognized, each with a unique pattern of speech-language features, underlying signature of neural changes, and associated disease aetiology (Gorno-Tempini et al., 2004, 2011). Because of the relatively focal topography of neurodegeneration in PPA, individuals experience a largely isolated decline in communicative function for several years. However, disease progression leads to the eventual emergence of more global dementia and/or degenerative motor syndromes (Harciarek et al., 2014).
Behavioural interventions for primary progressive aphasia
As a result of improved diagnostic precision, PPA is now identified with greater accuracy and frequency and, increasingly, patients and their families seek options for treatment. A robust literature documents the benefits of behavioural intervention for speech and language decline that occurs in stroke-induced aphasia (Brady et al., 2016); however, the treatment literature investigating the efficacy of rehabilitation in PPA is much more modest (Croot et al., 2009; Carthery-Goulart et al., 2013; Kortte and Rogalski, 2013; Rising, 2014; Jokel et al., 2014; Tippett et al., 2015). This is likely due to the relatively recent recognition of PPA as a clinical entity and to pessimism on the part of both clinicians and third party reimbursers regarding the utility of treatment in patients with neurodegenerative disease (Taylor et al., 2009). Further, most studies to date have not followed patients for a substantial period of time post-treatment to determine the longer-term outcomes of intervention (but see Henry et al., 2013; Meyer et al., 2018). As such, there is a critical need for research documenting the benefits conferred by speech-language treatment in patients with PPA and other progressive disorders, as well as the long-term outcomes from behavioural intervention in the context of ongoing neurodegeneration.
Existing research examining speech and language interventions in PPA has shown that targeted treatment approaches may have substantial benefit. Most of this work, however, has explored treatment for word retrieval, with the bulk of studies implementing treatment with individuals with the semantic variant of PPA and a growing number addressing treatment for the logopenic variant (Rising, 2014; Tippett et al., 2015). In contrast, behavioural treatment research in the non-fluent/agrammatic variant of PPA (nfvPPA) is quite limited (Duffy et al., 2014). In the current study, we sought to address this gap by implementing a targeted behavioural treatment for the core speech and language features that diminish communication abilities in individuals with nfvPPA.
Speech-language features and treatment research in non-fluent/agrammatic PPA
Diagnostic criteria for nfvPPA include the core features of agrammatism and/or apraxia of speech (Gorno-Tempini et al., 2011) and the syndrome is associated with damage to left posterior fronto-insular, premotor and striatal regions, as well as supplementary motor area (Grossman et al., 1996; Nestor et al., 2003; Gorno-Tempini et al., 2004, 2006; Ogar et al., 2007; Wilson et al., 2010a; Mandelli et al., 2016). Whereas isolated syntactic or speech motor deficits are sufficient for establishing the diagnosis, many individuals with this variant present with gradually worsening disruption of fluency caused by both linguistic and motoric deficits (Josephs et al., 2013; Santos-Santos et al., 2016). However, given that these deficits can occur in isolation, alternative diagnostic labels have been adopted by some clinicians and research groups. Those with isolated, progressive apraxia of speech have been alternatively characterized as having primary progressive apraxia of speech (PPAOS; Josephs et al., 2012) whereas those with isolated or predominant grammatical deficits have been classified as PPA-agrammatic (Mesulam et al., 2009). Additional cognitive-linguistic features stipulated by the diagnostic criteria, two of which must be present for diagnosis, include impaired syntactic comprehension, spared single-word comprehension, and spared object knowledge (Gorno-Tempini et al., 2011).
Speech-language treatment research in nfvPPA is limited, comprising studies investigating multi-component (Farrajota et al., 2012; Andrade-Calderón et al., 2015) or phased (Murray, 1998) training approaches aimed to improve general communicative function as well as interventions targeting specific skills. The bulk of these studies have investigated restitutive interventions for naming (Jokel et al., 2009; Marcotte and Ansaldo, 2010; Cotelli et al., 2014, 2016; Croot et al., 2015; Flanagan et al., 2016; Meyer et al., 2016, 2018; Hameister et al., 2017), with additional studies examining treatments for spelling (Tsapkini et al., 2014), phonological processing (Louis et al., 2001), and augmentative and alternative communication (Pattee et al., 2006; Fried-Oken et al., 2010). Findings are positive, with improvements noted for trained behaviours in most studies, generalized improvement to untrained items, exemplars or tasks noted in some studies (Louis et al., 2001; Cotelli et al., 2014, 2016; Tsapkini et al., 2014; Meyer et al., 2016), and maintenance effects observed in some cases, but inconsistently reported (Jokel et al., 2009; Cotelli et al., 2014, 2016; Tsapkini et al., 2014; Meyer et al., 2016, 2018).
Only a few studies have examined treatments addressing the core deficits of grammar and speech production in nfvPPA. One study (Schneider et al., 1996) trained a participant with nfvPPA to produce sentences containing a set of transitive verbs in future and past tenses, reporting generalization to untrained verbs and some maintenance at 3 months post-treatment. Another study implemented a brief errorless intervention targeting verb inflection and sentence production in a single nfvPPA case, observing improvement for trained and untrained sentences as well as maintenance at 1 month post-treatment (Machado et al., 2014). A constraint-induced treatment approach implemented with two nfvPPA participants resulted in improved production of grammatical structures, with maintenance of gains observed at 2 months post-treatment (Hameister et al., 2017). In a study targeting apraxia of speech in nfvPPA, an oral reading protocol was implemented with a single participant as a means to facilitate multisyllabic word production (Henry et al., 2013). Treatment resulted in a decrease in speech errors in untrained text as well as an increase in successfully self-corrected speech errors. Speech production in connected speech remained stable up to 1 year post-treatment. Together, these studies confirm that grammar and apraxia of speech may improve with treatment in nfvPPA; however, none addressed both the syntactic and motoric deficits that are the central features of this variant and all involved only one or two participants.
Script training as a treatment for speech production and fluency in aphasia and apraxia of speech
Script training, a technique that involves repeated practice of phrase or sentence-level material in the form of a monologue or dialogue, has been shown to improve speech production and fluency in individuals with aphasia (Holland et al., 2002; Youmans et al., 2005, 2011; Cherney et al., 2008; Lee et al., 2009; Bilda, 2011; Cherney, 2012; Goldberg et al., 2012) and apraxia of speech (Youmans et al., 2011) caused by stroke and is therefore a viable candidate approach for rehabilitation of communication deficits in nfvPPA. Script training may, in fact, be an ideal intervention as it has the potential to address both the core motoric (apraxia) and linguistic (agrammatism) deficits in nfvPPA. In individuals with apraxia of speech, script training has been shown to promote fluidity of speech, with a reduction in errors as well as reduced effortfulness of speech production overall (Youmans et al., 2011). With regard to grammar, previous literature on the effects of script training in aphasia supports the notion that improved syntactic production can be mediated by interventions other than traditional morphosyntactic or linguistically-motivated approaches that target syntax explicitly (Youmans et al., 2005; Cherney et al., 2008; Goldberg et al., 2012). This finding is consistent with the notion that improved grammar may result from exposure to and repetition of syntactically accurate productions, in lieu of explicit training of grammatical rules (Helm-Estabrooks et al., 1981; Helm-Estabrooks and Nicholas, 2000).
Script training has been implemented using a variety of training approaches with stroke patients, including a technique called ‘speech entrainment’ (Fridriksson et al., 2012). This procedure uses repeated practice of scripted material with an audiovisual model of an unimpaired speaker, which patients attempt to mimic in real time. An initial study in stroke patients found that speech entrainment facilitates fluent speech production in patients with Broca’s aphasia, and a subsequent study confirmed that the greatest improvements in fluency occurred in patients with damage to the left inferior frontal gyrus (pars opercularis and pars triangularis) (Fridriksson et al., 2015).
Current study
Despite positive findings in stroke patients with grammatical and motor speech deficits in the context of damage to left frontal regions, script training has not been systematically implemented as a therapeutic approach in nfvPPA. Nonetheless, the behavioural and anatomical congruence of Broca’s aphasia with nfvPPA supports the potential application of script training as a means to facilitate fluent speech production in this patient group. As such, we implemented a phase 1 study (Beeson and Robey, 2006) intended to explore the utility of script training via speech entrainment in nfvPPA. Additionally, we include a corroborative imaging study to examine the pattern of brain atrophy associated with responsiveness to this type of intervention in patients with neurodegenerative disease. We hypothesized that this treatment would result in improved speech production and fluency for trained content in individuals with nfvPPA. Further, we predicted that script training would confer a protective benefit against a backdrop of deteriorating speech and language, with trained scripts showing less decline than untrained topics up to 1 year post-treatment. We used structural MRI to examine the neural predictors of treatment gains by correlating pretreatment grey matter volumes with treatment effect sizes in regions of interest within the speech-language network.
Materials and methods
Participants
Ten individuals with mild-moderate non-fluent/agrammatic variant PPA were seen for assessment and treatment across two sites: the Aphasia Research and Treatment Lab at the University of Texas, Austin (n = 7) and the Memory and Aging Center at the University of California, San Francisco (UCSF) (n = 3). All participants gave written informed consent, and the study was approved by the institutional review boards at both institutions. Diagnosis of PPA was based on current clinical criteria (Gorno-Tempini et al., 2011) after a comprehensive neurological, neuropsychological (Kramer et al., 2003) and speech-language evaluation (Tables 1 and 2). To meet a diagnosis of the non-fluent/agrammatic variant, individuals were required to present with core features of (i) agrammatism in production (based on connected speech sample and standardized testing); and/or (ii) effortful, halting speech with features of apraxia of speech, as determined by a motor speech evaluation (Wertz et al., 1984). All participants presented with motor speech impairment. Specifically, all demonstrated features of apraxia of speech and 8 of 10 showed features of dysarthria. All but three participants demonstrated evidence of agrammatism in connected speech and/or on standardized testing. The remaining three participants demonstrated minimal agrammatism [score of 90% correct on the Northwestern Anagram Test (Weintraub et al., 2009), an assessment of expressive grammar, and spared grammar in connected speech]. Beyond nfvPPA diagnosis, the following inclusionary criteria were imposed: Mini-Mental State Examination (Folstein et al., 1975) score ≥15 and intact repetition of up to three syllables on the Western Aphasia Battery-Revised (Kertesz, 2006) repetition subtest. The resulting sample is consistent with the larger UCSF cohort of mild nfvPPA patients, most of whom have impairments of both motor speech and grammar, but a minority of whom present with isolated motoric (or, less commonly, grammatical) impairment in early stages of the disorder (Wilson et al., 2010b; Santos-Santos et al., 2016).
Demographic information and cognitive-linguistic test scores at pretreatment for nfvPPA participants
| Patient ID | NFV1 | NFV2 | NFV3 | NFV4 | NFV5 | NFV6 | NFV7 | NFV8 | NFV9 | NFV10 | Mean (SD) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Demographic | |||||||||||
| Age | 69 | 71 | 57 | 68 | 72 | 61 | 71 | 69 | 75 | 64 | 67.70 (5.5) |
| Gender | Male | Female | Male | Female | Female | Male | Female | Female | Female | Male | |
| Education (yrs) | 18 | 15 | 18 | 12 | 16 | 18 | 14 | 16 | 16 | 13 | 15.60 (2.1) |
| Handedness | Right | Right | Right | Right | Right | Right | Right | Right | Right | Right | |
| Mini-Mental State Examination (30) | 26 | 29 | 28 | 30 | 28 | 25 | 24 | 25 | 29 | 24 | 26.80 (2.1) |
| Mode of treatment | IP | TT | TT | IP | TT | IP | IP | IP | TT | TT | |
| Language and speech | |||||||||||
| Boston Naming Test (30 or 60) | 55/60 | 56/60 | 58/60 | 53/60 | 54/60 | 56/60 | 23/30 | 52/60 | 57/60 | 21/30 | 55.13 (2.0)/60 |
| Western Aphasia Battery | 22.00 (1.4)/30 | ||||||||||
| Information content (10) | 9 | 10 | 10 | 9 | 9 | 9 | 9 | 9 | 9 | 8 | 9.10 (0.6) |
| Fluency rating (10) | 5 | 5 | 9 | 9 | 5 | 5 | 5 | 6 | 5 | 5 | 5.90 (1.7) |
| Comprehension (200) | 200 | 184 | 199 | 192 | 200 | 189 | 192 | 178 | 200 | 200 | 193.40 (7.9) |
| Repetition (100) | 76 | 89 | 95 | 96 | 89 | 73 | 78 | 84 | 86 | 69 | 83.50 (9.2) |
| Naming (100) | 87 | 94 | 100 | 91 | 100 | 84 | 87 | 92 | 96 | 83 | 91.40 (6.2) |
| PPVT-short (16)a | 16 | 15 | 16 | 14 | – | 11 | 10 | 16 | 16 | 16 | 14.44 (2.4) |
| Working memory | |||||||||||
| Digit span forward | 4 | – | 6 | 8 | 4 | 5 | 5 | 5 | 5 | 4 | 5.11 (1.3) |
| Visuospatial function | |||||||||||
| Benson figure copy (17)a | 9 | 16 | 17 | 14 | 14 | 14 | 13 | 11 | 14 | 17 | 13.90 (2.5) |
| Visual memory | |||||||||||
| Benson figure recall (17)a | 5 | 12 | 15 | 7 | 14 | 11 | 8 | 7 | 14 | 12 | 10.50 (3.5) |
| Verbal memory | |||||||||||
| CVLT-SF Trials 1–4 (36)a | 18 | – | 25 | 30 | – | 18 | 26 | 19 | 31 | 25 | 24.00 (5.2) |
| CVLT-SF 30 s free recall (9)a | 6 | – | 6 | 9 | – | 4 | 8 | 6 | 9 | 7 | 6.88 (1.7) |
| CVLT-SF 10 min free recall (9)a | 6 | – | 6 | 7 | – | 5 | 8 | 5 | 9 | 8 | 6.75 (1.5) |
| Executive function | |||||||||||
| Digit span backward | 2 | – | 5 | 4 | 3 | 3 | 3 | 2 | 3 | 4 | 3.22 (1.0) |
| Modified Trails (lines per min)a | 7 | – | 28 | 3 | – | 23 | 19 | 8 | 31 | 5 | 15.42 (11.1) |
| Patient ID | NFV1 | NFV2 | NFV3 | NFV4 | NFV5 | NFV6 | NFV7 | NFV8 | NFV9 | NFV10 | Mean (SD) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Demographic | |||||||||||
| Age | 69 | 71 | 57 | 68 | 72 | 61 | 71 | 69 | 75 | 64 | 67.70 (5.5) |
| Gender | Male | Female | Male | Female | Female | Male | Female | Female | Female | Male | |
| Education (yrs) | 18 | 15 | 18 | 12 | 16 | 18 | 14 | 16 | 16 | 13 | 15.60 (2.1) |
| Handedness | Right | Right | Right | Right | Right | Right | Right | Right | Right | Right | |
| Mini-Mental State Examination (30) | 26 | 29 | 28 | 30 | 28 | 25 | 24 | 25 | 29 | 24 | 26.80 (2.1) |
| Mode of treatment | IP | TT | TT | IP | TT | IP | IP | IP | TT | TT | |
| Language and speech | |||||||||||
| Boston Naming Test (30 or 60) | 55/60 | 56/60 | 58/60 | 53/60 | 54/60 | 56/60 | 23/30 | 52/60 | 57/60 | 21/30 | 55.13 (2.0)/60 |
| Western Aphasia Battery | 22.00 (1.4)/30 | ||||||||||
| Information content (10) | 9 | 10 | 10 | 9 | 9 | 9 | 9 | 9 | 9 | 8 | 9.10 (0.6) |
| Fluency rating (10) | 5 | 5 | 9 | 9 | 5 | 5 | 5 | 6 | 5 | 5 | 5.90 (1.7) |
| Comprehension (200) | 200 | 184 | 199 | 192 | 200 | 189 | 192 | 178 | 200 | 200 | 193.40 (7.9) |
| Repetition (100) | 76 | 89 | 95 | 96 | 89 | 73 | 78 | 84 | 86 | 69 | 83.50 (9.2) |
| Naming (100) | 87 | 94 | 100 | 91 | 100 | 84 | 87 | 92 | 96 | 83 | 91.40 (6.2) |
| PPVT-short (16)a | 16 | 15 | 16 | 14 | – | 11 | 10 | 16 | 16 | 16 | 14.44 (2.4) |
| Working memory | |||||||||||
| Digit span forward | 4 | – | 6 | 8 | 4 | 5 | 5 | 5 | 5 | 4 | 5.11 (1.3) |
| Visuospatial function | |||||||||||
| Benson figure copy (17)a | 9 | 16 | 17 | 14 | 14 | 14 | 13 | 11 | 14 | 17 | 13.90 (2.5) |
| Visual memory | |||||||||||
| Benson figure recall (17)a | 5 | 12 | 15 | 7 | 14 | 11 | 8 | 7 | 14 | 12 | 10.50 (3.5) |
| Verbal memory | |||||||||||
| CVLT-SF Trials 1–4 (36)a | 18 | – | 25 | 30 | – | 18 | 26 | 19 | 31 | 25 | 24.00 (5.2) |
| CVLT-SF 30 s free recall (9)a | 6 | – | 6 | 9 | – | 4 | 8 | 6 | 9 | 7 | 6.88 (1.7) |
| CVLT-SF 10 min free recall (9)a | 6 | – | 6 | 7 | – | 5 | 8 | 5 | 9 | 8 | 6.75 (1.5) |
| Executive function | |||||||||||
| Digit span backward | 2 | – | 5 | 4 | 3 | 3 | 3 | 2 | 3 | 4 | 3.22 (1.0) |
| Modified Trails (lines per min)a | 7 | – | 28 | 3 | – | 23 | 19 | 8 | 31 | 5 | 15.42 (11.1) |
aFrom Kramer et al. (2003).
Amb = ambidextrous; CVLT-SF = California Verbal Learning Test- UCSF version; F = female; IP = in-person treatment; M = male; PPVT = Peabody Picture Vocabulary Test; TT = teletherapy; WAB = Western Aphasia Battery-Revised.
Demographic information and cognitive-linguistic test scores at pretreatment for nfvPPA participants
| Patient ID | NFV1 | NFV2 | NFV3 | NFV4 | NFV5 | NFV6 | NFV7 | NFV8 | NFV9 | NFV10 | Mean (SD) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Demographic | |||||||||||
| Age | 69 | 71 | 57 | 68 | 72 | 61 | 71 | 69 | 75 | 64 | 67.70 (5.5) |
| Gender | Male | Female | Male | Female | Female | Male | Female | Female | Female | Male | |
| Education (yrs) | 18 | 15 | 18 | 12 | 16 | 18 | 14 | 16 | 16 | 13 | 15.60 (2.1) |
| Handedness | Right | Right | Right | Right | Right | Right | Right | Right | Right | Right | |
| Mini-Mental State Examination (30) | 26 | 29 | 28 | 30 | 28 | 25 | 24 | 25 | 29 | 24 | 26.80 (2.1) |
| Mode of treatment | IP | TT | TT | IP | TT | IP | IP | IP | TT | TT | |
| Language and speech | |||||||||||
| Boston Naming Test (30 or 60) | 55/60 | 56/60 | 58/60 | 53/60 | 54/60 | 56/60 | 23/30 | 52/60 | 57/60 | 21/30 | 55.13 (2.0)/60 |
| Western Aphasia Battery | 22.00 (1.4)/30 | ||||||||||
| Information content (10) | 9 | 10 | 10 | 9 | 9 | 9 | 9 | 9 | 9 | 8 | 9.10 (0.6) |
| Fluency rating (10) | 5 | 5 | 9 | 9 | 5 | 5 | 5 | 6 | 5 | 5 | 5.90 (1.7) |
| Comprehension (200) | 200 | 184 | 199 | 192 | 200 | 189 | 192 | 178 | 200 | 200 | 193.40 (7.9) |
| Repetition (100) | 76 | 89 | 95 | 96 | 89 | 73 | 78 | 84 | 86 | 69 | 83.50 (9.2) |
| Naming (100) | 87 | 94 | 100 | 91 | 100 | 84 | 87 | 92 | 96 | 83 | 91.40 (6.2) |
| PPVT-short (16)a | 16 | 15 | 16 | 14 | – | 11 | 10 | 16 | 16 | 16 | 14.44 (2.4) |
| Working memory | |||||||||||
| Digit span forward | 4 | – | 6 | 8 | 4 | 5 | 5 | 5 | 5 | 4 | 5.11 (1.3) |
| Visuospatial function | |||||||||||
| Benson figure copy (17)a | 9 | 16 | 17 | 14 | 14 | 14 | 13 | 11 | 14 | 17 | 13.90 (2.5) |
| Visual memory | |||||||||||
| Benson figure recall (17)a | 5 | 12 | 15 | 7 | 14 | 11 | 8 | 7 | 14 | 12 | 10.50 (3.5) |
| Verbal memory | |||||||||||
| CVLT-SF Trials 1–4 (36)a | 18 | – | 25 | 30 | – | 18 | 26 | 19 | 31 | 25 | 24.00 (5.2) |
| CVLT-SF 30 s free recall (9)a | 6 | – | 6 | 9 | – | 4 | 8 | 6 | 9 | 7 | 6.88 (1.7) |
| CVLT-SF 10 min free recall (9)a | 6 | – | 6 | 7 | – | 5 | 8 | 5 | 9 | 8 | 6.75 (1.5) |
| Executive function | |||||||||||
| Digit span backward | 2 | – | 5 | 4 | 3 | 3 | 3 | 2 | 3 | 4 | 3.22 (1.0) |
| Modified Trails (lines per min)a | 7 | – | 28 | 3 | – | 23 | 19 | 8 | 31 | 5 | 15.42 (11.1) |
| Patient ID | NFV1 | NFV2 | NFV3 | NFV4 | NFV5 | NFV6 | NFV7 | NFV8 | NFV9 | NFV10 | Mean (SD) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Demographic | |||||||||||
| Age | 69 | 71 | 57 | 68 | 72 | 61 | 71 | 69 | 75 | 64 | 67.70 (5.5) |
| Gender | Male | Female | Male | Female | Female | Male | Female | Female | Female | Male | |
| Education (yrs) | 18 | 15 | 18 | 12 | 16 | 18 | 14 | 16 | 16 | 13 | 15.60 (2.1) |
| Handedness | Right | Right | Right | Right | Right | Right | Right | Right | Right | Right | |
| Mini-Mental State Examination (30) | 26 | 29 | 28 | 30 | 28 | 25 | 24 | 25 | 29 | 24 | 26.80 (2.1) |
| Mode of treatment | IP | TT | TT | IP | TT | IP | IP | IP | TT | TT | |
| Language and speech | |||||||||||
| Boston Naming Test (30 or 60) | 55/60 | 56/60 | 58/60 | 53/60 | 54/60 | 56/60 | 23/30 | 52/60 | 57/60 | 21/30 | 55.13 (2.0)/60 |
| Western Aphasia Battery | 22.00 (1.4)/30 | ||||||||||
| Information content (10) | 9 | 10 | 10 | 9 | 9 | 9 | 9 | 9 | 9 | 8 | 9.10 (0.6) |
| Fluency rating (10) | 5 | 5 | 9 | 9 | 5 | 5 | 5 | 6 | 5 | 5 | 5.90 (1.7) |
| Comprehension (200) | 200 | 184 | 199 | 192 | 200 | 189 | 192 | 178 | 200 | 200 | 193.40 (7.9) |
| Repetition (100) | 76 | 89 | 95 | 96 | 89 | 73 | 78 | 84 | 86 | 69 | 83.50 (9.2) |
| Naming (100) | 87 | 94 | 100 | 91 | 100 | 84 | 87 | 92 | 96 | 83 | 91.40 (6.2) |
| PPVT-short (16)a | 16 | 15 | 16 | 14 | – | 11 | 10 | 16 | 16 | 16 | 14.44 (2.4) |
| Working memory | |||||||||||
| Digit span forward | 4 | – | 6 | 8 | 4 | 5 | 5 | 5 | 5 | 4 | 5.11 (1.3) |
| Visuospatial function | |||||||||||
| Benson figure copy (17)a | 9 | 16 | 17 | 14 | 14 | 14 | 13 | 11 | 14 | 17 | 13.90 (2.5) |
| Visual memory | |||||||||||
| Benson figure recall (17)a | 5 | 12 | 15 | 7 | 14 | 11 | 8 | 7 | 14 | 12 | 10.50 (3.5) |
| Verbal memory | |||||||||||
| CVLT-SF Trials 1–4 (36)a | 18 | – | 25 | 30 | – | 18 | 26 | 19 | 31 | 25 | 24.00 (5.2) |
| CVLT-SF 30 s free recall (9)a | 6 | – | 6 | 9 | – | 4 | 8 | 6 | 9 | 7 | 6.88 (1.7) |
| CVLT-SF 10 min free recall (9)a | 6 | – | 6 | 7 | – | 5 | 8 | 5 | 9 | 8 | 6.75 (1.5) |
| Executive function | |||||||||||
| Digit span backward | 2 | – | 5 | 4 | 3 | 3 | 3 | 2 | 3 | 4 | 3.22 (1.0) |
| Modified Trails (lines per min)a | 7 | – | 28 | 3 | – | 23 | 19 | 8 | 31 | 5 | 15.42 (11.1) |
aFrom Kramer et al. (2003).
Amb = ambidextrous; CVLT-SF = California Verbal Learning Test- UCSF version; F = female; IP = in-person treatment; M = male; PPVT = Peabody Picture Vocabulary Test; TT = teletherapy; WAB = Western Aphasia Battery-Revised.
Speech-language test performance at pre- and post-treatment and treatment effect sizes
| Patient ID | NFV1 | NFV2 | NFV3 | NFV4 | NFV5 | NFV6 | NFV7 | NFV8 | NFV9 | NFV10 | Mean (SD) | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| WAB AQ, /100 | Pre | 80.6 | 85.0 | 96.9 | 92.6 | 85.8 | 78.3 | 80.2 | 83.0 | 84.4 | 76.2 | 84.3 (6.4) |
| Post | 85.5 | 85.6 | 97.7 | 92.9 | 85.4 | 81.8 | 80.0 | 78.8 | 89.0 | 80.2 | 85.7 (6.1) | |
| AOS ratinga (0 = none; 7 = profound) | Pre | 5 | 3 | 3 | 4 | 6 | 2 | 4 | 2 | 4 | 4 | 3.7 (1.3) |
| Post | 6 | 4 | 4 | 5 | 6 | 2 | 5 | 3 | 4 | 4 | 4.3 (1.3) | |
| Dysarthria ratinga (0 = none; 7 = profound) | Pre | 4 | 0 | 4 | 4 | 5 | 2 | 3 | 0 | 4 | 3 | 2.9 (1.7) |
| Post | 5 | 0 | 4 | 5 | 5 | 2 | 3 | 0 | 4 | 3 | 3.1 (1.9) | |
| NAT, % | Pre | 40.0 | 53.3 | 90.0 | 90.0 | 50.0 | N/A | 36.7 | 66.7 | 90.0 | 56.7 | 63.7 (21.5) |
| Post | 70.0 | 73.3 | 100.0 | 83.3 | 73.3 | 50.0 | 53.3 | 100.0 | 93.3 | 46.7 | 74.3 (20.0) | |
| Treatment effect size (d-statistics) | Trained scripts | 9.6 | 15.0 | 11.8 | 9.9 | 8.7 | 7.3 | 16.0 | 0.6 | 7.4 | 23.2 | 11.0 (6.1) |
| Untrained scripts | −5.9 | 3.6 | 2.6 | 2.7 | 1.4 | 1.1 | 4.8 | −1.0 | 0.1 | −0.4 | 0.89 (3.0) | |
| Patient ID | NFV1 | NFV2 | NFV3 | NFV4 | NFV5 | NFV6 | NFV7 | NFV8 | NFV9 | NFV10 | Mean (SD) | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| WAB AQ, /100 | Pre | 80.6 | 85.0 | 96.9 | 92.6 | 85.8 | 78.3 | 80.2 | 83.0 | 84.4 | 76.2 | 84.3 (6.4) |
| Post | 85.5 | 85.6 | 97.7 | 92.9 | 85.4 | 81.8 | 80.0 | 78.8 | 89.0 | 80.2 | 85.7 (6.1) | |
| AOS ratinga (0 = none; 7 = profound) | Pre | 5 | 3 | 3 | 4 | 6 | 2 | 4 | 2 | 4 | 4 | 3.7 (1.3) |
| Post | 6 | 4 | 4 | 5 | 6 | 2 | 5 | 3 | 4 | 4 | 4.3 (1.3) | |
| Dysarthria ratinga (0 = none; 7 = profound) | Pre | 4 | 0 | 4 | 4 | 5 | 2 | 3 | 0 | 4 | 3 | 2.9 (1.7) |
| Post | 5 | 0 | 4 | 5 | 5 | 2 | 3 | 0 | 4 | 3 | 3.1 (1.9) | |
| NAT, % | Pre | 40.0 | 53.3 | 90.0 | 90.0 | 50.0 | N/A | 36.7 | 66.7 | 90.0 | 56.7 | 63.7 (21.5) |
| Post | 70.0 | 73.3 | 100.0 | 83.3 | 73.3 | 50.0 | 53.3 | 100.0 | 93.3 | 46.7 | 74.3 (20.0) | |
| Treatment effect size (d-statistics) | Trained scripts | 9.6 | 15.0 | 11.8 | 9.9 | 8.7 | 7.3 | 16.0 | 0.6 | 7.4 | 23.2 | 11.0 (6.1) |
| Untrained scripts | −5.9 | 3.6 | 2.6 | 2.7 | 1.4 | 1.1 | 4.8 | −1.0 | 0.1 | −0.4 | 0.89 (3.0) | |
aFrom Wertz et al. (1984).
AOS = apraxia of speech; NAT = Northwestern Anagram Test; WAB AQ = Western Aphasia Battery Aphasia Quotient.
Speech-language test performance at pre- and post-treatment and treatment effect sizes
| Patient ID | NFV1 | NFV2 | NFV3 | NFV4 | NFV5 | NFV6 | NFV7 | NFV8 | NFV9 | NFV10 | Mean (SD) | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| WAB AQ, /100 | Pre | 80.6 | 85.0 | 96.9 | 92.6 | 85.8 | 78.3 | 80.2 | 83.0 | 84.4 | 76.2 | 84.3 (6.4) |
| Post | 85.5 | 85.6 | 97.7 | 92.9 | 85.4 | 81.8 | 80.0 | 78.8 | 89.0 | 80.2 | 85.7 (6.1) | |
| AOS ratinga (0 = none; 7 = profound) | Pre | 5 | 3 | 3 | 4 | 6 | 2 | 4 | 2 | 4 | 4 | 3.7 (1.3) |
| Post | 6 | 4 | 4 | 5 | 6 | 2 | 5 | 3 | 4 | 4 | 4.3 (1.3) | |
| Dysarthria ratinga (0 = none; 7 = profound) | Pre | 4 | 0 | 4 | 4 | 5 | 2 | 3 | 0 | 4 | 3 | 2.9 (1.7) |
| Post | 5 | 0 | 4 | 5 | 5 | 2 | 3 | 0 | 4 | 3 | 3.1 (1.9) | |
| NAT, % | Pre | 40.0 | 53.3 | 90.0 | 90.0 | 50.0 | N/A | 36.7 | 66.7 | 90.0 | 56.7 | 63.7 (21.5) |
| Post | 70.0 | 73.3 | 100.0 | 83.3 | 73.3 | 50.0 | 53.3 | 100.0 | 93.3 | 46.7 | 74.3 (20.0) | |
| Treatment effect size (d-statistics) | Trained scripts | 9.6 | 15.0 | 11.8 | 9.9 | 8.7 | 7.3 | 16.0 | 0.6 | 7.4 | 23.2 | 11.0 (6.1) |
| Untrained scripts | −5.9 | 3.6 | 2.6 | 2.7 | 1.4 | 1.1 | 4.8 | −1.0 | 0.1 | −0.4 | 0.89 (3.0) | |
| Patient ID | NFV1 | NFV2 | NFV3 | NFV4 | NFV5 | NFV6 | NFV7 | NFV8 | NFV9 | NFV10 | Mean (SD) | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| WAB AQ, /100 | Pre | 80.6 | 85.0 | 96.9 | 92.6 | 85.8 | 78.3 | 80.2 | 83.0 | 84.4 | 76.2 | 84.3 (6.4) |
| Post | 85.5 | 85.6 | 97.7 | 92.9 | 85.4 | 81.8 | 80.0 | 78.8 | 89.0 | 80.2 | 85.7 (6.1) | |
| AOS ratinga (0 = none; 7 = profound) | Pre | 5 | 3 | 3 | 4 | 6 | 2 | 4 | 2 | 4 | 4 | 3.7 (1.3) |
| Post | 6 | 4 | 4 | 5 | 6 | 2 | 5 | 3 | 4 | 4 | 4.3 (1.3) | |
| Dysarthria ratinga (0 = none; 7 = profound) | Pre | 4 | 0 | 4 | 4 | 5 | 2 | 3 | 0 | 4 | 3 | 2.9 (1.7) |
| Post | 5 | 0 | 4 | 5 | 5 | 2 | 3 | 0 | 4 | 3 | 3.1 (1.9) | |
| NAT, % | Pre | 40.0 | 53.3 | 90.0 | 90.0 | 50.0 | N/A | 36.7 | 66.7 | 90.0 | 56.7 | 63.7 (21.5) |
| Post | 70.0 | 73.3 | 100.0 | 83.3 | 73.3 | 50.0 | 53.3 | 100.0 | 93.3 | 46.7 | 74.3 (20.0) | |
| Treatment effect size (d-statistics) | Trained scripts | 9.6 | 15.0 | 11.8 | 9.9 | 8.7 | 7.3 | 16.0 | 0.6 | 7.4 | 23.2 | 11.0 (6.1) |
| Untrained scripts | −5.9 | 3.6 | 2.6 | 2.7 | 1.4 | 1.1 | 4.8 | −1.0 | 0.1 | −0.4 | 0.89 (3.0) | |
aFrom Wertz et al. (1984).
AOS = apraxia of speech; NAT = Northwestern Anagram Test; WAB AQ = Western Aphasia Battery Aphasia Quotient.
Neurologically intact controls for the imaging portion of the study included 60 individuals with no history of neurological or psychological illness who were scanned at the University of Texas, Austin (n = 30) or UCSF (n = 30). Whole brain voxel-based morphometry analysis revealed atrophy in the nfvPPA patients in left inferior frontal gyrus (pars opercularis and triangularis), middle frontal gyrus, precentral gyrus, insula, caudate, putamen, and supplementary motor area as well as right middle and inferior frontal gyri and supplementary motor area (Fig. 1) relative to healthy controls (n = 60).
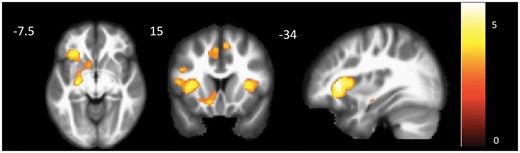
Results of whole brain voxel-based morphometry showing areas of significant atrophy in participants with nfvPPA (n = 9) relative to healthy controls (n = 60). The map was derived by conducting a two-group t-test, with age, sex, total grey matter volume, and scanner as covariates (P < 0.001, uncorrected). Colour bar represents t-values. One participant with nfvPPA could not be scanned because of contraindications.
Experimental design
Video-implemented script training for aphasia (VISTA) was used with all participants, consisting of (i) twice weekly (45 min to 1 h) sessions with a clinician (H.H. or S.G.) targeting articulatory and grammatical aspects of script production, as well as memorization and conversational usage of scripted material (see Box 1 for treatment details and example scripts); and (ii) speech entrainment homework with personalized scripts. The VISTA training hierarchy, used for in-session treatment with the clinician, moved from structured tasks (e.g. reading scripted sentences aloud and targeting accuracy and intelligibility of production) to more functional tasks (e.g. producing scripted sentences from memory in conversation with novel conversational partners), in order to promote memorization and generalized conversational usage. Speech sound errors were addressed through targeted articulation practice during therapy via drills and visual placement cues.
Box 1 Hierarchy of tasks used in treatment sessions to promote memorization and conversational usage of scripts
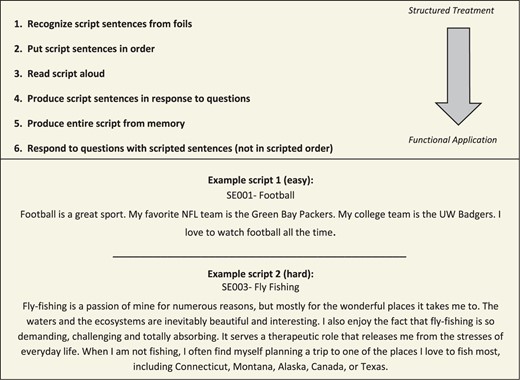
Training hierarchy and examples of easier and more challenging scripts.
Note that feedback regarding articulatory and grammatical accuracy, including modelling of correct production, was provided during all production tasks (steps 3–6). Step 6 was conducted with a naïve communication partner during the second training session for each script, in order to promote generalized conversational usage.
Six functional, personalized script topics were selected by participants and script content (four to seven sentences) was generated via a collaborative process with the clinician. Four scripts were randomly selected for training, and two scripts remained untrained. Scripts were balanced both within and between trained and untrained sets for number of words, number of sentences, number of complex (multisyllabic) words, mean words per sentence, and mean syllables per word. Video stimuli were created for home practice, which showed a healthy speaker (mouth only) producing each script. Articulatory gestures were exaggerated to provide salient visual cues for production. Syntactic and articulatory difficulty of scripts and rate of speech for videos were tailored to each participant (see examples of an easier and more challenging script, Box 1). To provide a challenging yet feasible target speech rate, video stimuli were tailored to the individual’s maximum attainable rate, which was determined from picture description and oral passage reading tasks. Each script was trained for a minimum of two and a maximum of three sessions with the clinician (until 90% of scripted words were produced correctly and intelligibly).
For home practice, participants were instructed to attempt to speak in unison with the videotaped speaker (using an iPad and headphones) in real time for a minimum of 30 min of daily practice with the current script. Additionally, participants practiced articulating a list of two to four scripted words that were difficult for them to articulate during the previous session with the clinician. Five of 10 participants received treatment via teletherapy, as they lived in locations that were remote from the research sites, making traveling for each treatment session impractical. After treatment ended, participants retained their training videos. Ongoing practice was encouraged, and participants were asked to track their practice via a written log, which was collected at follow-up assessments. Follow-up testing was conducted at 3 months, 6 months, and 1 year post-treatment.
Outcome measures and statistical analysis
The primary outcome measure was per cent correct, intelligible words produced in response to a prompt question posed by the clinician (e.g. ‘Tell me about ___.’) relative to the script target. Effect sizes (d-statistics, mean post-treatment score minus mean pretreatment score divided by pretreatment standard deviation (Beeson and Robey, 2006) were calculated for both trained and untrained scripts to serve as a metric of individual response to treatment and for correlation with imaging variables. Additional outcome measures of interest were grammatical errors produced per 100 words and overall intelligibility (per cent intelligible words produced in response to the clinician’s prompt, irrespective of the script target). These secondary outcomes were considered as they have the potential to capture generalized improvement in speech and grammar regardless of a participant’s ability to memorize and reproduce scripted topics verbatim. For group analyses as well as individual d-statistics, pretreatment score was calculated as the average of two pretreatment probes, whereas the post-treatment measure was calculated as the average of two probes collected after training on all scripts was completed. Follow-up measures reflect a single probe. See Supplementary material for details regarding reliability of coding and assessment of treatment fidelity.
The distribution of difference scores for paired samples tests did not meet the assumption of normality. As such, we used the exactRankTests package (Hothorn and Hornik, 2017) in R (version 3.3.2; 2016) to conduct non-parametric paired permutation tests using a complete enumeration of all possible pairings. For these analyses, pretreatment performance was compared to post-treatment performance and each follow-up time point (3 months, 6 months and 1 year post-treatment) for (i) primary and secondary outcome measures; and (ii) performance on standardized tests, including a measure of overall language impairment [the Western Aphasia Battery Aphasia Quotient (AQ; Kertesz, 2006)] and a non-verbal test of expressive grammar [the Northwestern Anagram Test (Weintraub et al., 2009)]. Additionally, performance on trained versus untrained scripts was compared at each time point to determine the specificity of treatment effects. One-tailed permutation tests were used to examine performance on trained scripts over time and to compare trained versus untrained scripts, as we predicted a substantial, lasting and significantly greater (relative to untrained topics) improvement for trained topics. Two-tailed permutation tests were used to assess change on untrained scripts and standardized tests, as generalization effects (and maintenance thereof) were less predictable. Exact significance levels are reported as well as t-values. Each outcome measure was considered independent and orthogonal to the others, with different expectations and outcomes; however, a Bonferroni correction was applied across time points within each outcome measure, with adjusted alpha of P = 0.0125.
Post-treatment survey
An in-house 21-item survey was administered post-treatment to all participants with nfvPPA and to spouses or caregivers when possible (Box 2). Survey questions queried perceptions of participants’ ability to speak fluently and in grammatical sentences, without pauses and errors, in scripted and non-scripted contexts. The ability to detect and correct speech errors in these contexts was also queried, as was perception of overall speaking ability, stress level during conversation, and feelings of confidence or frustration during communication exchanges with familiar versus unfamiliar individuals. Each item was rated on a seven-point scale from ‘a lot worse’ (−3) to ‘a lot better’ (+3).
Box 2 Post-treatment survey items
| Since completing treatment, how would you rate your: | |||
| Q1 | Ability to speak smoothly and without errors in practiced scripts | Q12 | Ability to communicate thoughts |
| Q2 | Ability to speak smoothly and without errors during normal conversations | Q13 | Overall speaking ability |
| Q3 | Ability to speak in complete sentences, using all the “little” grammatical words in practiced scripts | Q14 | Stress level during conversation |
| Q4 | Ability to speak in complete sentences, using all the “little” grammatical words in normal conversation | Q15 | Overall comfort level while speaking |
| Q5 | Articulation during practiced scripts (ability to clearly say the sounds within a word) | Q16 | Confidence in communication with your primary communication partner (e.g. spouse) |
| Q6 | Articulation during normal conversation (ability to clearly say the sounds within a word) | Q17 | Confidence in communication with familiar people |
| Q7 | Overall number of hesitations or pauses while producing scripts | Q18 | Confidence in communication with unfamiliar people |
| Q8 | Overall number of hesitations or pauses in normal conversation | Q19 | Frustration level during communication exchanges with primary communication partner |
| Q9 | Ability to speak in time with video model during speech entrainment | Q20 | Frustration level during communication exchanges with familiar people |
| Q10 | Ability to detect errors in speech | Q21 | Frustration level during communication exchanges with unfamiliar people |
| Q11 | Ability to correct speech errors when they occur | ||
| Since completing treatment, how would you rate your: | |||
| Q1 | Ability to speak smoothly and without errors in practiced scripts | Q12 | Ability to communicate thoughts |
| Q2 | Ability to speak smoothly and without errors during normal conversations | Q13 | Overall speaking ability |
| Q3 | Ability to speak in complete sentences, using all the “little” grammatical words in practiced scripts | Q14 | Stress level during conversation |
| Q4 | Ability to speak in complete sentences, using all the “little” grammatical words in normal conversation | Q15 | Overall comfort level while speaking |
| Q5 | Articulation during practiced scripts (ability to clearly say the sounds within a word) | Q16 | Confidence in communication with your primary communication partner (e.g. spouse) |
| Q6 | Articulation during normal conversation (ability to clearly say the sounds within a word) | Q17 | Confidence in communication with familiar people |
| Q7 | Overall number of hesitations or pauses while producing scripts | Q18 | Confidence in communication with unfamiliar people |
| Q8 | Overall number of hesitations or pauses in normal conversation | Q19 | Frustration level during communication exchanges with primary communication partner |
| Q9 | Ability to speak in time with video model during speech entrainment | Q20 | Frustration level during communication exchanges with familiar people |
| Q10 | Ability to detect errors in speech | Q21 | Frustration level during communication exchanges with unfamiliar people |
| Q11 | Ability to correct speech errors when they occur | ||
See also Fig. 3.
Box 2 Post-treatment survey items
| Since completing treatment, how would you rate your: | |||
| Q1 | Ability to speak smoothly and without errors in practiced scripts | Q12 | Ability to communicate thoughts |
| Q2 | Ability to speak smoothly and without errors during normal conversations | Q13 | Overall speaking ability |
| Q3 | Ability to speak in complete sentences, using all the “little” grammatical words in practiced scripts | Q14 | Stress level during conversation |
| Q4 | Ability to speak in complete sentences, using all the “little” grammatical words in normal conversation | Q15 | Overall comfort level while speaking |
| Q5 | Articulation during practiced scripts (ability to clearly say the sounds within a word) | Q16 | Confidence in communication with your primary communication partner (e.g. spouse) |
| Q6 | Articulation during normal conversation (ability to clearly say the sounds within a word) | Q17 | Confidence in communication with familiar people |
| Q7 | Overall number of hesitations or pauses while producing scripts | Q18 | Confidence in communication with unfamiliar people |
| Q8 | Overall number of hesitations or pauses in normal conversation | Q19 | Frustration level during communication exchanges with primary communication partner |
| Q9 | Ability to speak in time with video model during speech entrainment | Q20 | Frustration level during communication exchanges with familiar people |
| Q10 | Ability to detect errors in speech | Q21 | Frustration level during communication exchanges with unfamiliar people |
| Q11 | Ability to correct speech errors when they occur | ||
| Since completing treatment, how would you rate your: | |||
| Q1 | Ability to speak smoothly and without errors in practiced scripts | Q12 | Ability to communicate thoughts |
| Q2 | Ability to speak smoothly and without errors during normal conversations | Q13 | Overall speaking ability |
| Q3 | Ability to speak in complete sentences, using all the “little” grammatical words in practiced scripts | Q14 | Stress level during conversation |
| Q4 | Ability to speak in complete sentences, using all the “little” grammatical words in normal conversation | Q15 | Overall comfort level while speaking |
| Q5 | Articulation during practiced scripts (ability to clearly say the sounds within a word) | Q16 | Confidence in communication with your primary communication partner (e.g. spouse) |
| Q6 | Articulation during normal conversation (ability to clearly say the sounds within a word) | Q17 | Confidence in communication with familiar people |
| Q7 | Overall number of hesitations or pauses while producing scripts | Q18 | Confidence in communication with unfamiliar people |
| Q8 | Overall number of hesitations or pauses in normal conversation | Q19 | Frustration level during communication exchanges with primary communication partner |
| Q9 | Ability to speak in time with video model during speech entrainment | Q20 | Frustration level during communication exchanges with familiar people |
| Q10 | Ability to detect errors in speech | Q21 | Frustration level during communication exchanges with unfamiliar people |
| Q11 | Ability to correct speech errors when they occur | ||
See also Fig. 3.
Imaging methods
Structural MRI scans were obtained for participants with nfvPPA when possible (n = 9) at the University of Texas, Austin (n = 4) or the UCSF (n = 5) and healthy control scans were available from historical datasets at each site (30 per site). T1-weighted 3D magnetization prepared rapid acquisition gradient echo (MPRAGE) sequences were collected on a Siemens Skyra 3 T scanner (UT Austin) or Siemens Trio 3 T scanner (UCSF). See Supplementary material for scanning parameters.
Voxel-based morphometry was used to characterize patterns of regional atrophy in participants with nfvPPA relative to the 60 age-matched healthy controls in the whole brain (Fig. 1) and within a previously identified speech production network. Structural T1 scans were segmented into grey matter, white matter, and CSF using the VBM8 toolbox (http://www.neuro.uni-jena.de/vbm/) for SPM8 within MATLAB version 2014b (The MathWorks, Inc.). Images were bias-corrected, then registered to Montreal Neurological Institute (MNI) space through an affine and a non-linear deformation. The non-linear deformation parameters were calculated with the high dimensional diffeomorphic anatomical registration through exponentiated lie (DARTEL) algorithm and the predefined templates within the SPM DARTEL toolbox (Ashburner, 2007). The voxel-based morphometry analysis was conducted using modulated grey matter images, with voxel values multiplied by Jacobian determinants derived from the spatial normalization in order to preserve the total amount of grey matter from the original images. Modulated images were smoothed with a Gaussian kernel (8 mm full-width at half-maximum).
NfvPPA is a disorder of network-based degeneration (Seeley et al., 2009), with the earliest and most prominent site of atrophy (i.e. the ‘epicentre’) located in the left inferior frontal gyrus. In a previous multimodal imaging study, we used seed-based resting-state functional connectivity analysis to identify an inferior frontal gyrus-anchored functional network that showed both connectivity in healthy individuals and selective degeneration in individuals with nfvPPA (Mandelli et al., 2016). The network comprised left frontal, parietal, temporal, insular, and striatal regions as well as homotopic right hemisphere regions and the bilateral supplementary motor area. In the current study, we investigated grey matter atrophy within this network in the nfvPPA group relative to healthy controls. To do so, a mask was created by thresholding the healthy control network from our previous study at t > 8.75, cluster size >100. Within this mask, a two-group t-test was conducted with age, sex, total grey matter volume, and scanner as covariates (thresholded at P < 0.001, uncorrected). Additionally, regions of interest were created from the 11 discrete clusters comprising the inferior frontal gyrus-seeded network mask, and mean grey matter volumes from regions of interest were examined as predictors of treatment response in nfvPPA patients. Regions of interest included: left striatum, left cuneus, left inferior frontal gyrus, left inferior parietal lobe, left middle/inferior temporal gyrus, right caudate, right inferior frontal gyrus, right inferior temporal gyrus, right postcentral gyrus, right precuneus, and supplementary motor area. Mean volumes from regions of interest were extracted for each participant and converted to z-scores relative to healthy controls from the relevant scanning site (UT Austin or UCSF). Partial correlations, with Western Aphasia Battery AQ included as a covariate to control for aphasia severity, were conducted to examine the relation between region of interest volume z-score and treatment effect size (d-statistic). Bonferroni correction was applied, with adjusted alpha of P = 0.0045.
Results
Demographic information and cognitive scores for the 10 nfvPPA participants are presented in Table 1. Individuals who received treatment via teletherapy did not differ significantly in overall disease severity (Mini-Mental State Examination score) or for demographic factors (age or education) relative to the face-to-face treatment group (independent samples t-tests, P-values > 0.05), so outcomes were examined for the combined group of traditional and teletherapy participants for all subsequent analyses. Below, we present results indicating immediate treatment effects, stability and specificity of these effects, patient and caregiver reports of treatment-induced change, and neural predictors of treatment response.
Treatment effects from pre- to post-treatment
Individual response to treatment was robust [mean d-statistic = 11.0, standard deviation (SD) = 6.1, Table 2], with substantial effect sizes for trained scripts for all participants but one (Participant NFV8), who demonstrated a small effect (d = 0.6). Small or even negative effects were observed for untrained scripts (mean = 0.89, SD = 3.0). Group data depicting primary and secondary outcome measures and performance on standardized tests are displayed in Fig. 2 (see Supplementary Table 1 for descriptive statistics and Supplementary Tables 2–5 for statistical details). Permutation tests for paired data revealed significant improvement for the primary outcome measure (per cent correct, intelligible scripted words produced) for trained (t = −8.76, P = 0.001) scripts at post-treatment (Fig. 2A). With regard to secondary outcome measures, overall per cent intelligibility significantly improved for trained (t = −2.02, P = 0.006) as well as untrained (t = −1.03, P = 0.012) topics at post-treatment (Fig. 2B) and there was a significant reduction in grammatical errors for trained scripts only (t = 2.10, P = 0.002; Fig. 2C). Because only a subset of participants demonstrated grammatical impairment pretreatment, we conducted an additional test with the subset of (n = 7) grammatically impaired patients, which confirmed a significant improvement for this subgroup (t = 2.06, P = 0.016). Small improvements were observed on the Northwestern Anagram Test (t = −2.60, P = 0.023) and the Western Aphasia Battery AQ (t = −1.54, P = 0.043) from pre- to post-treatment (Fig. 2D); however, these did not survive correction for multiple comparisons.
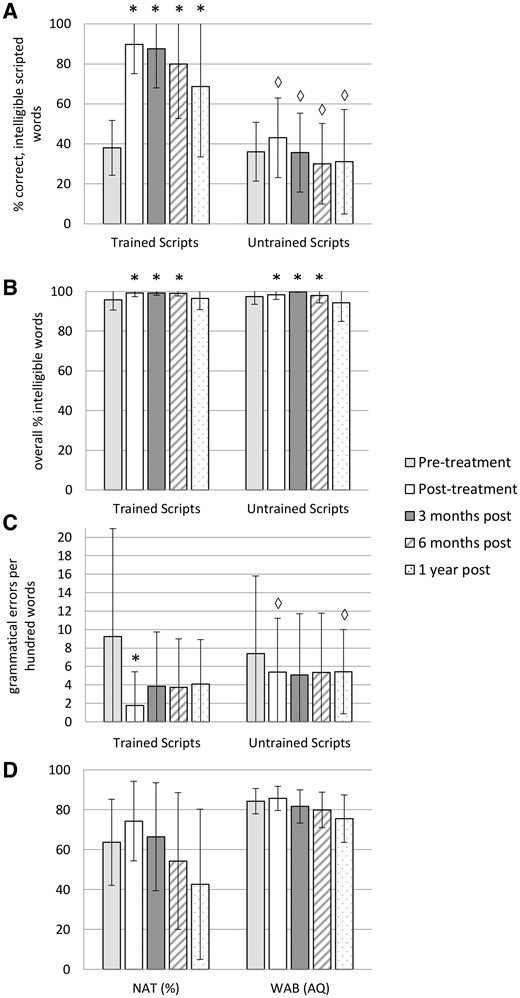
Primary and secondary treatment outcome measures and standardized tests at each time point. Primary outcome measure: (A) Per cent correct, intelligible scripted words for trained and untrained topics. Secondary outcome measures: (B) Overall per cent intelligible words and (C) Number of grammatical errors per 100 words for trained and untrained topics. (D) Standardized test performance. NAT = Northwestern Anagram Test; WAB = Western Aphasia Battery AQ. Values represent group means. Error bars show standard deviation, and are included for descriptive purposes but not for inference, as significance derived by paired permutation test. Asterisk = significantly different from pretreatment within trained or untrained scripts (P < 0.0125); diamond = significantly different from trained scripts at the same time point (P < 0.0125).
Stability of treatment effects at follow-up time points through 1 year post-treatment
Pretreatment performance was compared with follow-up performance at 3 months, 6 months, and 1 year post-treatment for the primary outcome measure (correct, intelligible scripted words), secondary outcome measures (overall per cent intelligibility and grammatical errors per 100 words), and standardized tests (the Northwestern Anagram Test and the Western Aphasia Battery AQ). Follow-up data through 1 year post-treatment were available for all participants except one, who became ill between the 6-month and 1-year follow-up and was unable to continue with the study.
The significant improvement for the primary outcome measure on trained scripts was maintained at 3 months (t = −7.20, P = 0.002), 6 months (t = −4.56, P = 0.002), and 1 year (t = −2.54, P = 0.012) post-treatment (Fig. 2A). Per cent intelligibility for trained and untrained scripts continued to be significantly greater than pretreatment at the 3-month (trained scripts t = −2.09, P = 0.006; untrained scripts t = −2.12, P = 0.002) and 6-month (trained scripts t = −1.92, P = 0.002; untrained scripts t = −1.88, P = 0.012) follow-ups, but was not significantly different at 1 year post-treatment (Fig. 2B; Supplementary Table 3). Grammatical errors per 100 words were reduced relative to pretreatment for trained and untrained scripts at all follow-ups; however, the reductions were not significant with correction for multiple comparisons (Fig. 2C; Supplementary Table 4). The Northwestern Anagram Test and Western Aphasia Battery AQ were not significantly different from pretreatment at any follow-up assessment, but did show a steady decline after treatment ended (Fig. 2D; Supplementary Table 5).
Specificity of treatment effects and the relation between continued home practice and maintenance
A direct comparison of trained versus untrained scripts for all outcome measures revealed no difference in performance at pretreatment. At post-treatment and each follow-up time point, performance on trained topics was significantly better than untrained topics for the primary outcome measure (post-treatment t = 8.36, P = 0.002; 3-month t = 7.16, P = 0.002, 6-month t = 7.27, P = 0.002; 1-year t = 4.24, P = 0.004; Fig. 2A). Overall intelligibility was not significantly different for trained relative to untrained topics at post-treatment or any follow-up time point (Fig. 2B; Supplementary Table 3). By contrast, number of grammatical errors per 100 words (Fig. 2C) was significantly reduced at post-treatment (t = −2.40, P = 0.001) and one year post-treatment (t = −2.03, P = 0.012; Fig. 2C, Supplementary Table 4). When examined in the subgroup of (n = 7) patients with detectable grammatical impairment at pretreatment, the difference between trained and untrained scripts was only significant at post-treatment (t = −2.27, P = 0.008).
To examine the relation between continued home practice (after the completion of clinician-administered treatment) and treatment effects over time, we examined the strength of the correlation between treatment change score (relative to post-treatment score) and number of home practice sessions completed at each follow-up. The correlation was not significant for trained or untrained scripts at any time point (P-values > 0.05).
Post-treatment survey data
The 21-item survey was administered to all participants with nfvPPA and to patients’ spouses or caregivers when possible (n = 7/10). Each item was rated on a scale from ‘a lot worse’, with a rating of −3 to ‘a lot better’ with a rating of +3 (Fig. 3 and Box 2). The mean rating across items for participants with nfvPPA was 1.21, between ‘somewhat better’ and ‘better’. The mean spouse/caregiver rating was 0.95, corresponding to ‘somewhat better’ overall. Patients rated the following items with a score of ‘better’ or higher, on average: ability to speak in grammatical sentences in practiced scripts; articulation during practiced scripts; ability to speak in time with the video model; and ability to correct speech errors when they occur. Patients rated the following items with a score between ‘somewhat better’ and ‘better’, on average: ability to speak smoothly and without errors in practiced scripts; ability to speak smoothly and without errors during normal conversations; ability to speak in complete sentences during normal conversation; articulation during normal conversation; number of hesitations or pauses in scripts or normal conversation; ability to detect errors in speech; confidence and frustration level in communication with primary partner (e.g. spouse), and frustration level during communication exchanges with other familiar people.
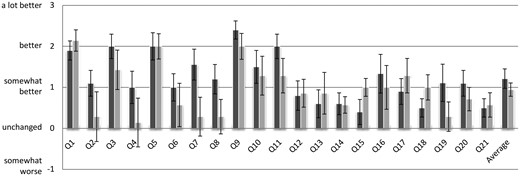
Mean ratings from post-treatment survey. Mean survey responses from patients (n = 10; dark grey) and spouses/caregivers (n = 7; light grey). Error bars represent standard error. See also Box 2.
Neuroimaging
Figure 4 depicts the inferior frontal gyrus-seeded resting state functional MRI network identified in our previous study of healthy controls (Mandelli et al., 2016). Within that network, regions of significant atrophy in the cohort of nfvPPA participants included bilateral supplementary motor area, left inferior frontal gyrus, left precentral and postcentral gyri, left putamen, and right inferior frontal gyrus and precentral gyrus (see Supplementary Table 6 for details). Analyses examining the relation between treatment effect size and mean grey matter volumes for regions of interest representing peak clusters within the healthy control inferior frontal gyrus-anchored network (Mandelli et al., 2016) revealed a significant partial correlation (controlling for aphasia severity) for the left middle/inferior temporal gyrus region of interest only (r = 0.875, P = 0.002; Fig. 4 and Supplementary Table 7).
Discussion
Evidence regarding the immediate and long-term benefits of motoric and cognitive-linguistic interventions in neurodegenerative disease is mixed. There are promising findings supporting motor training to improve current level of function and even slow the progression of motor symptoms in disorders such as degenerative ataxia (Aranca et al., 2016), Parkinson’s disease (Mak et al., 2017), and progressive supranuclear palsy (Clerici et al., 2017). Findings regarding the utility of non-linguistic cognitive interventions in dementia are inconsistent, with some evidence supporting group cognitive stimulation treatments and individualized cognitive rehabilitation programmes, but little support for training programmes targeting specific cognitive domains (Livingston et al., 2017). With regard to language rehabilitation specifically, treatment studies in logopenic and semantic variants of PPA document promising outcomes, albeit with limited evidence for generalization and maintenance of gains (Carthery-Goulart et al., 2013; Rising, 2014; Tippett et al., 2015). Among the PPA clinical syndromes, nfvPPA alone presents with both linguistic and motoric deficits. As such, this population provides a unique testing ground for the efficacy of behavioural intervention, with important ramifications for clinical management of patients with a variety of neurodegenerative disorders and associated symptoms.
To our knowledge, this is the first group study to examine treatment targeting speech production and fluency in nfvPPA and one of a limited number of studies (Henry et al., 2013; Meyer et al., 2018) to examine treatment outcomes for up to 1 year post-treatment in patients with speech and language impairment caused by neurodegenerative disease. Outcomes indicate that script training with speech entrainment is an efficacious treatment in this patient group, with both objective and subjective benefits to participants. Immediately following treatment, we observed improvement on our primary outcome measure of correct, intelligible words produced as well as a reduction in grammatical errors for trained scripts. We also documented a small but significant increase in overall per cent intelligibility for both trained and untrained topics. The potential for change on this measure was limited by relatively preserved intelligibility at pretreatment and therefore, the utility of VISTA for improving intelligibility will be better addressed in a larger sample with more variability in baseline speech intelligibility. It is noteworthy that the participant from our sample who was least intelligible at pretreatment (NFV 1; 85% intelligible) improved by 15% for trained and 7% for untrained topics post-treatment, suggesting that VISTA may result in clinically significant gains in intelligibility for those with a greater degree of impairment.
Post-treatment surveys confirmed that objective treatment gains were mirrored by subjective benefits, as perceived by patients and caregivers, on a range of communication skills (e.g. speaking grammatically) and also by a sense of reduced frustration and improved confidence during communication attempts for some patients. In fact, we acknowledge that reduced frustration and heightened confidence may have been contributing factors in patients’ improvement on other, more objective, outcome measures; however, we are not able to discern to what extent. We attribute the robust treatment response to the multifaceted nature of the VISTA protocol. The multilevel stimulation (from articulatory placement cueing to conversational practice) afforded by the in-session training hierarchy, combined with the intensive audiovisual homework practice, facilitated gains in both motoric (e.g. intelligibility) and linguistic (e.g. grammaticality) domains, with carry-over to functional communication contexts.
Whereas the group-level analyses document significant and lasting benefit as a result of VISTA, it is also important to consider response to treatment at the individual level, with particular attention paid to any individuals who showed a less robust response to treatment. Nine of our 10 participants showed robust effect sizes for the primary outcome measure, whereas one participant (Participant NFV8) showed only a small effect (d = 0.6). This is likely due, in part, to participant factors and, in part, to the manner in which the d-statistic was calculated for this study. With regard to participant factors, Participant NFV8 demonstrated a greater level of anxiety during script probes relative to other participants, and was more likely to abandon attempts to produce scripts verbatim, instead providing non-scripted or even unrelated information. Additionally, Participant NFV8 demonstrated dysexecutive behaviours (stimulus boundness, distractibility) during training sessions and presented with limb apraxia, which may have affected her ability to manipulate the iPad used for script practice. She also had the lowest Western Aphasia Battery comprehension score of the group, which could have influenced her ability to respond appropriately to probe questions. It is important to note that Participant NFV8 reached criterion performance of at least 90% correct intelligible words for three of her four scripts (and 83% correct on her fourth script); however, her performance dropped gradually but considerably once training on each script stopped (e.g. from 90.9% correct intelligible words after two training sessions on script 1 to 50% correct intelligible words produced after all scripts were trained). As such, our method of calculating the effect size, which used probe performance once all training was complete, reflected lower scores than were achieved during training. Lastly, Participant NFV8 demonstrated greater variability in pretreatment probe performance, which also effectively reduced the magnitude of the d-statistic. Despite a small effect on the primary outcome measure, this participant did show a sizeable improvement on the Northwestern Anagram Test (from 66.7% to 100% correct) from pre- to post-treatment, suggesting that script training may have had some benefit for syntactic production overall. Future research should examine cognitive and other participant factors that may affect responsiveness to intervention, in order to inform treatment candidacy decision-making and optimize the training approach for patients with specific pretreatment cognitive-linguistic profiles.
Group follow-up testing data confirmed our prediction that rehearsal of scripted material may result in a prophylactic benefit for trained material, as scripted speech samples showed maintenance of correct, intelligible word production up to 1 year post-treatment. A direct comparison of performance on trained versus untrained scripts revealed the specificity of the training effect for the primary outcome measure, with worse performance at all time points for untrained topics. Per cent intelligibility, by contrast, did not differ significantly in trained versus untrained topics at any time point and grammatical errors per 100 words differed significantly at only a subset of follow-up time points, suggesting broad benefit to untrained topics on these measures that do not rely on script memorization. It is important to note that untrained script performance was not significantly worse than baseline for any metric over the 1-year follow-up period. Northwestern Anagram Test scores and Western Aphasia Battery AQ also remained relatively stable during the follow-up period. Together, these findings suggest that treatment may have helped to stabilize speech and language, despite disease progression.
In the interest of promoting lasting benefit from our treatment efforts, we did not withdraw treatment materials from participants at the end of the structured intervention period and, in fact, encouraged them to continue to practice their trained scripts and to record the frequency with which they practiced. Individuals varied greatly in the amount of practice that they undertook post-treatment, from no practice at all to multiple practice sessions per week. Surprisingly, the reported frequency of practice did not correlate at any follow-up time point with treatment change scores (relative to post-treatment). As such, we cannot conclude that there was a significant relationship between post-treatment practice frequency and maintenance of treatment gains after formal treatment ended. In fact, one of our most impaired participants (NFV1) reported no post-treatment practice, yet performed significantly better than pretreatment at both 3- and 6-month follow-ups (pretreatment score: 40% correct, intelligible words; post-treatment: 98%; 3 months post-treatment: 92%, and 6 months post-treatment: 69%), only declining relative to pretreatment at his 1 year evaluation (21% correct, intelligible words). We interpret this finding at the group level with caution, as this is a rather small sample and we were reliant on patient self-report to determine frequency of post-treatment practice. Future studies should digitally track practice frequency and duration (Fridriksson et al., 2015) in order to examine the relation between practice dosage during and after the formal treatment phase and immediate and long-term treatment effects.
Our imaging findings corroborate the lesion profile (pars opercularis and triangularis of the left inferior frontal gyrus) associated with responsiveness to speech entrainment in a previous study investigating aphasia caused by stroke (Fridriksson et al., 2015). Atrophy in our nfvPPA cohort encompassed additional regions within networks supporting motor speech (Bohland and Guenther, 2006; Guenther, 2006; Tourville and Guenther, 2011) and syntax (Wilson et al., 2010a, 2016), including basal ganglia, bilateral supplementary motor area, and right frontal regions. Region of interest analyses examining specific nodes within the inferior frontal gyrus-anchored speech production network revealed that pretreatment grey matter volumes in a left middle/inferior temporal gyrus region of interest were predictive of the magnitude of treatment response. Neuropsychological and functional MRI studies have documented a role for posterior temporal regions in syntactic processing, including both comprehension and production (Dronkers et al., 2004; Wilson et al., 2010a, 2016; Menenti et al., 2011; Segaert et al., 2012; Thompson and Meltzer-Asscher, 2014; Blank et al., 2016). As such, improved grammaticality of output with VISTA training may be mediated by largely non-atrophic middle and inferior temporal regions that support syntactic production.
Additionally, previous work has implicated left posterior middle temporal gyrus in speech production during speech entrainment (Fridriksson et al., 2012) and during rehearsal of speech following an audiovisual model (Venezia et al., 2016). These studies suggest a significant role for posterior middle temporal gyrus in a visuo-motor speech network that serves to facilitate fluent speech production in the context of damage to the dorsal auditory-to-motor pathway. Specifically, this alternative pathway is thought to complement auditory targets with visual targets to enhance speech motor control. A significant correlation between VISTA treatment outcomes and posterior middle/inferior temporal volumes may reflect compensatory reliance on an alternative, visually-mediated pathway for facilitation and preservation of motor speech function in patients with deterioration of dorsal perisylvian structures. An alternative hypothesis might be that this region’s predictive power reflects a greater potential for benefit in patients with relative sparing of word-finding ability pretreatment, as this region has been consistently implicated in word retrieval (DeLeon et al., 2007; Price, 2012; Race et al., 2013; Herbet et al., 2016; Hope and Price, 2016). To address this possibility, we conducted a post hoc correlation analysis examining the relation between treatment effect size and pretreatment Boston Naming Test score. The correlation was not significant (r = −0.621, P = 0.055) and was negative, reflecting greater effect size with lower naming score. In fact, our most impaired participant on the Boston Naming Test (Participant NFV10, Boston Naming Test score = 70%) showed the greatest treatment effect size (d = 23.23). As such, we cannot conclude that this region’s role in treatment response is related solely to spared naming ability pretreatment.
It is noteworthy that we did not find significant correlations between treatment effect size and regions most closely linked with syntactic and motor functions in the literature. We note that that left inferior frontal gyrus (r = 0.603, P = 0.057) and inferior parietal lobule (r = 0.579, P = 0.066) were borderline significant (without Bonferroni correction) and supplementary motor area also showed a moderately strong, but non-significant relationship (r = 0.528, P = 0.089) with treatment effect size. It is reasonable to hypothesize that the integrity of these regions does likely play a role in treatment response and that, in a larger sample, significant relationships may emerge.
The imaging analyses for the current study focused on grey matter alterations within a previously established, inferior frontal gyrus-anchored, speech production network. Undoubtedly, white matter degeneration also contributes to the profile of deficits observed in nfvPPA. Specifically, alterations in white matter have been documented in left dorsal frontoparietal and frontotemporal language tracts (Galantucci et al., 2011) and damage to particular tracts has been associated with certain motoric and linguistic deficits. Broadly, alterations within white matter tracts underlying left frontal regions have been associated with speech sound distortions using voxel-based morphometry (Wilson et al., 2010b) and changes in diffusion tensor imaging (DTI) metrics in tracts connecting Brodmann areas 44/6 and the supplementary motor area have been associated with motor speech errors (Mandelli et al., 2014). By contrast, syntax comprehension and production deficits have been associated with the integrity of the superior longitudinal fasciculus/arcuate fasciculus (Wilson et al., 2011; Mandelli et al., 2014). Future studies examining structural predictors of treatment response should include DTI metrics, in order to address whether the integrity of specific tracts contributes to treatment outcomes above and beyond grey matter volumes. Additionally, future studies might include pre- to post-treatment functional neuroimaging, as has been conducted in a small number of prior PPA treatment studies (Dressel et al., 2010; Marcotte and Ansaldo, 2010; Beeson et al., 2011; Jokel et al., 2016). These studies have documented changes in activation patterns for language tasks in patients at post-treatment which, together, implicate recruitment of anatomically spared left and right hemisphere regions. Comparisons of pre- and post-treatment task-based functional MRI as well as resting-state functional connectivity patterns may provide important insights regarding reorganization of the language network and compensatory recruitment of both left and right hemisphere regions following treatment in nfvPPA.
In addition to these anatomical considerations, there are relevant findings from other populations that may shed light on the mechanism behind improved and maintained speech and language with VISTA training. In individuals who stutter, auditory and visual choral speech have well-documented fluency inducing effects (Cherry and Sayers, 1956; Andrews et al., 1982; Kalinowski et al., 2000). This has been attributed to activation of an alternative speech signal mediated by auditory input, visual input, or both (Kalinowski et al., 2000). In stroke patients with aphasia and apraxia of speech, script training has been hypothesized to increase automaticity of speech production via overlearning of motoric gestures and linguistic content (Youmans et al., 2005). Given the preservation of automatic speech (e.g. counting, reciting days of the week) in individuals with aphasia and apraxia of speech (Dronkers, 1996; Lum and Ellis, 1999), a treatment that promotes automaticity could potentially offer a protective benefit in the face of ongoing neurodegeneration. There is also the possibility that choral practice with a healthy speaker may serve not only to provide a correct auditory and visual model for imitation, but may also ‘mask’ the errorful feedback of the patient’s own speech. Accordingly, in some individuals with apraxia of speech caused by stroke, provision of masked auditory feedback has been shown to increase speech fluency (Jacks and Haley, 2015).
In summary, we report the immediate and longer-term benefit of speech-language intervention in a group of patients with non-fluent/agrammatic PPA. Ours is the first group study to implement treatment addressing the core syntactic and motoric deficits that compromise communication in this patient group. It is also one of the first to follow individuals with PPA up to 1 year post-treatment, with findings supporting the utility of behavioural intervention not only for its immediate value, but also for long-term prophylactic benefit. This finding has broad ramifications for clinical service provision in these patients as well as those with other neurodegenerative syndromes (e.g. Alzheimer’s disease, Parkinson’s disease, etc.), who have been historically underserved by rehabilitation specialists and for whom reimbursement for treatment continues to be limited. The current group of nfvPPA participants was in the mild-moderate stages of disease severity and, as such, the utility of this intervention in more impaired participants will need to be addressed via future research. With disease progression, and progressively limited verbal output, an increasing emphasis on non-verbal communication is appropriate, necessitating a shift toward multimodality communication as well as augmentative and alternative communication (Pattee et al., 2006; Fried-Oken et al., 2010). Future studies should investigate the full continuum of approaches, including restitutive and compensatory interventions, to best meet the needs of patients at different stages in the disease process.
Acknowledgments
We thank members of the UT Austin Aphasia Research and Treatment Lab and the UCSF Memory and Aging Center, who contributed to patient assessment and care, and especially to Laura Herrera, Sarah Alanis, and Madison Kurtz, who conducted speech sample transcription and coding, as well as reliability and fidelity analyses. We also thank Gregory Hixon for statistical consultation. Finally, we wish to thank all of our participants with PPA for the time and effort that they have devoted to our research.
Funding
This work was funded by grants from the National Institutes of Health (M.H., NIDCD R01 DC016291), (M.H., NIDCD R03 DC013403), (M.GT., NINDS R01 NS050915), (M.GT., NIDCD K24 DC015544), (S.W., NIDCD R01 DC013270), (S.W., NIDCD R21 DC016080), (B.M., NIA P01 AG019724), (B.M., NIA P50 AG023501), (A.B., NINDS U54 NS092089), (A.B., NIA R01 AG038791) (J.F., NIDCD P50 DC014664) and the Darrell K Royal Research Fund for Alzheimer's Disease (M.H.).
Supplementary material
Supplementary material is available at Brain online.
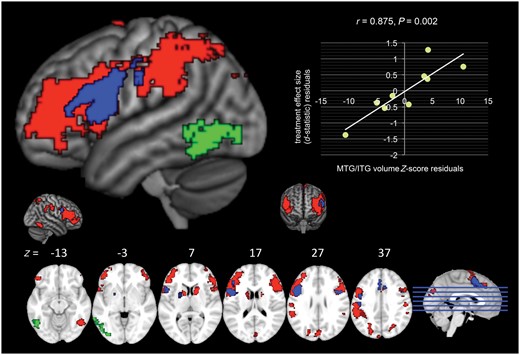
Volumetric analyses within the inferior frontal gyrus-seeded network. The healthy control inferior frontal gyrus-seeded network is depicted (red, green, and blue; Mandelli et al., 2016). Within that network, regions of significant atrophy in nfvPPA patients relative to healthy controls are indicated in blue (two-group t-test with age, sex, total gray matter volume, and scanner as covariates, P < 0.001, uncorrected) and the left middle/inferior temporal gyrus region of interest that significantly predicted treatment response (d-statistic, controlling for aphasia severity using Western Aphasia Battery AQ) is indicated in green.
Abbreviations
- nfvPPA
non-fluent/agrammatic PPA
- PPA
primary progressive aphasia
- VISTA
video-implemented script training for aphasia
References


{kind=link}
{kind=link}
{kind=link}
{kind=link}