





Abstract
Defining the duration of infectivity of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) has major implications for public health and infection control practice in healthcare facilities. Early in the pandemic, most hospitals required 2 negative RT-PCR tests before discontinuing isolation in patients with Covid-19. Many patients, however, have persistently positive RT-PCR tests for weeks to months following clinical recovery, and multiple studies now indicate that these generally do not reflect replication-competent virus. SARS-CoV-2 appears to be most contagious around the time of symptom onset, and infectivity rapidly decreases thereafter to near-zero after about 10 days in mild-moderately ill patients and 15 days in severely-critically ill and immunocompromised patients. The longest interval associated with replication-competent virus thus far is 20 days from symptom onset. This review summarizes evidence-to-date on the duration of infectivity of SARS-CoV-2, and how this has informed evolving public health recommendations on when it is safe to discontinue isolation precautions.
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the virus that causes Covid-19, has infected millions of people worldwide. Understanding the duration of SARS-CoV-2 infectivity has major implications for public health and infection control efforts. Prematurely releasing patients from isolation risks fueling transmission. Unnecessarily prolonging isolation, however, is frustrating for patients, consumes personal protective equipment, can delay procedures and other medical care, locks up scarce private and airborne infection isolation rooms, separates patients from social support, and may impede discharge. Policies that permit a timely but safe return to work for infected healthcare workers are also critical, particularly in hospitals facing staffing shortages. Furthermore, repeated RT-PCR testing for clearance consumes testing supplies and repeated nasopharyngeal swabs can cause nontrivial discomfort.
In this article, we review the current knowledge about the duration of SARS-CoV-2 transmissibility and how this has informed evolving recommendations from the World Health Organization (WHO) and U.S. Centers for Disease Control and Prevention (CDC).
INCUBATION PERIOD AND PEAK VIRAL LOAD
The median incubation period for SARS-CoV-2 is 4–5 days, with an interquartile range of 2–7 days [1, 2]. Approximately 98% of infected individuals who develop symptoms do so within 12 days [3]. Viral RNA levels are detectable in the respiratory tract 2–3 days before symptoms appear, peak at symptom onset, and decline over the following 7–8 days in most patients [4–8]. The capacity of asymptomatic and presymptomatic people to transmit virus prior to symptom onset is well documented [9–13]. SARS-CoV-2 therefore appears to have similar transmission dynamics to influenza, which is also contagious before and through several days after symptom onset [14–16].
DURATION OF PCR POSITIVITY
Early in the pandemic, WHO and CDC recommended test-based clearance with at least two negative RT-PCR tests for patients with Covid-19. This strategy, however, can lead to prolonged isolation, as some patients have positive RT-PCR assays for weeks if not months [17–22]. Sicker patients tend to have detectable RNA for longer periods, but prolonged PCR positivity also occurs in mildly ill and asymptomatic individuals [6, 8, 23–28]. The duration of PCR positivity appears to be longer in lower respiratory tract versus upper respiratory tract samples, as well as in stool samples [26, 29–32]. In addition, some patients recover from Covid-19, have two negative tests, and then test positive again even in the absence of new symptoms [33, 34].
INTERPRETING PCR TEST RESULTS: CYCLE THRESHOLDS AND NUCLEIC ACID QUANTITY
While PCR tests are reported as a binary result, the cycle threshold (Ct) value—the number of PCR cycles required for the sample fluorescence to exceed a predefined threshold—provides additional useful information. The Ct value is inversely related to the amount of nucleic acid present in the sample, such that every increase in Ct value of ~3.3 corresponds to a 10-fold reduction in the amount of nucleic acid [35]. Most SARS-CoV-2 PCR assays use a Ct cutoff of <40 for positivity. Patients in the early stages of infection usually have Ct values of 20–30 or less [36]. Ct values tend to increase thereafter, reflecting progressively lower amounts of viral RNA as the immune response clears the infection.
Ct values must be interpreted with caution as they do not reflect a true viral load, which requires standardization using reference curves. As such, they are not directly comparable across assays [37]. Furthermore, differences in specimen collection quality and reaction conditions can introduce further variation [38, 39]. This imprecision in PCR testing is most apparent when the amount of viral nucleic acid at the sampling site approaches the limit of detection for the assay and is the most common reason for why some patients alternate between testing negative and testing positive. Lastly, only traditional real-time PCR assays produce a Ct value; assays that use isothermal amplification do not product a Ct value and nested PCR assays are not designed for quantitative interpretation [40].
ASSESSING DURATION of INFECTIVITY by CELL CULTURE
It is now clear that persistent RNA detection does not necessarily translate into viable virus that can infect others. Subgenomic RNA fragments associate tightly with intracellular vesicles that protect them from degradation by host enzymes, which may explain why PCR tests are persistently positive in many patients [41]. The ability of SARS-CoV-2 to replicate in cultured cells is a better surrogate for infectivity. In a hamster study, for example, transmissibility of SARS-CoV-2 correlated with detection of infectious virus by culture, but not by RT-PCR positivity alone [42]. The possibility of human transmission despite nonculturable virus cannot be ruled out, since no study has attempted to link the presence of culturable virus directly to infectivity in humans. However, an increasing body of evidence suggests that time from symptom onset and Ct values are both useful proxies for infectivity. Notably, SARS-CoV-2 viral culture is not used in routine practice, as it can only be performed by specialized laboratories that meet minimum standards for biosafety.
Table 1 summarizes the evidence that persistently positive SARS-CoV-2 RNA PCRs are due to residual viral “debris” rather than replication-competent virus. The first study to make this suggestion was an analysis of 9 hospitalized patients with mild-moderate disease [6]. RNA was detectable by PCR for weeks after onset of symptoms in some patients; however, virus was only isolated by culture during the first week of symptoms and could not be cultured from any samples taken >8 days following symptom onset.
Summary of Studies Assessing Duration of SARS-CoV-2 Infectivity Based on Viral Cell Culture or Secondary Infection Rates
| Study (Country) | Population | Primary findings |
|---|---|---|
| Wolfel et al. [6] (Germany) | 9 young to middle-aged patients with mild disease | • Peak viral load prior to day 5 after symptom onset |
| • Virus unable to be cultured after day 8 from respiratory samples despite ongoing high viral load | ||
| • Virus unable to be cultured from stool, even with high viral load | ||
| U.S. Centers for Disease Control and Prevention [43] (U.S.) | Per CDC, data generated from adults across a variety of age groups and with varying severity of illness (unspecified number of patients) | • Virus unable to be cultured more than 9 days after symptom onset |
| • Attempts to culture virus from upper respiratory specimens largely unsuccessful when Ct values >33–35 | ||
| • Among patients who continue to have detectable RNA in upper respiratory specimens following clincal illness, concentrations are generally in the range at which replication-competent virus has not been reliably isolated | ||
| Young et al. [44] Singapore | 100 hospitalized patients (20 requiring supplemental oxygen and 12 requiring mechanical ventilation | • Viral culture unsuccessful in all PCR-positive samples with Ct values >30 |
| • 90% of all samples taken after day 14 from symptom onset had Ct values >30 | ||
| La Scola et al. [45] (France) | 183 PCR-positive samples (174 nasopharyngeal, 9 sputum) from 155 patients (unknown severity of illness) | • PCR tests positive for up to 20 days after symptom onset, but virus unable to be cultured after day 8 |
| • Samples with CT values 13–17 all led to positive culture | ||
| • No virus was successfully cultured when Ct values were ≥34 | ||
| Million et al. [46] (France) | 11 hospitalized PCR-positive patients in whom daily cultures were attempted past 10 days | • Virus unable to be cultured after day 10 |
| Bullard et al. [47] (Canada) | 90 PCR-positive nasopharyngeal or endotracheal aspirate samples taken through day 21 after symptom onset (unknown number of patients and severity of illness) | • Virus unable to be cultured after day 8 from symptom onset, or when Ct values were >24 |
| • Probability of culturing virus highest between days one and five and peaked on day 3 | ||
| • Each 1 unit increase in Ct value correlated with 32% decrease in odds of culturing virus | ||
| Liu et al. [25] (Taiwan) | 1 PCR-positive patient with mild febrile illness | • PCR positive through day 63 after symptom onset, but virus unable to be cultured after 18 days |
| van Kampen et al. [48] (Netherlands) | 690 upper and lower respiratory samples taken from 129 hospitalized patients with severe or critical illness, including 30 immunosuppresed patients | • Median duration of infectious shedding by viral culture = 8 days after symptom onset (IQR 5–11 days, maximum 20 days) |
| • Probability of obtaining infectious virus fell to <5% after 15 days from symptom onset | ||
| • Detection of viral RNA by PCR exceeded detection by culture | ||
| Cheng et al. [49] (Taiwan) | 100 patients with Covid-19 (mostly mild disease) | • Amongst 2761 close contacts, secondary attack rate was 0.7% amongst 1818 people who had contact within 5 days of symptom onset and 0% amongst 852 people who had contact ≥6 days after symptom onset |
| Lu et al. [50] (China) | 87 patients hospitalized patients with Covid-19, discharged after recovery and 2 consecutive negative PCR swabs, and then tested positive again within 2 weeks | • Viral cell culture and full-length genome sequencing unsuccessful in all cases |
| Korean Centers for Disease Control and Prevention [51] (South Korea) | 285 patients who recovered from Covid-19, tested negative, and then tested postive again by PCR (on average 45 days after initial symptom onset) | • Viral cell culture negative in 108 cases |
| • Ct values for re-postive tests >30 in 89.5% of cases | ||
| • 0% transmission to 790 contacts during re-positive period |
| Study (Country) | Population | Primary findings |
|---|---|---|
| Wolfel et al. [6] (Germany) | 9 young to middle-aged patients with mild disease | • Peak viral load prior to day 5 after symptom onset |
| • Virus unable to be cultured after day 8 from respiratory samples despite ongoing high viral load | ||
| • Virus unable to be cultured from stool, even with high viral load | ||
| U.S. Centers for Disease Control and Prevention [43] (U.S.) | Per CDC, data generated from adults across a variety of age groups and with varying severity of illness (unspecified number of patients) | • Virus unable to be cultured more than 9 days after symptom onset |
| • Attempts to culture virus from upper respiratory specimens largely unsuccessful when Ct values >33–35 | ||
| • Among patients who continue to have detectable RNA in upper respiratory specimens following clincal illness, concentrations are generally in the range at which replication-competent virus has not been reliably isolated | ||
| Young et al. [44] Singapore | 100 hospitalized patients (20 requiring supplemental oxygen and 12 requiring mechanical ventilation | • Viral culture unsuccessful in all PCR-positive samples with Ct values >30 |
| • 90% of all samples taken after day 14 from symptom onset had Ct values >30 | ||
| La Scola et al. [45] (France) | 183 PCR-positive samples (174 nasopharyngeal, 9 sputum) from 155 patients (unknown severity of illness) | • PCR tests positive for up to 20 days after symptom onset, but virus unable to be cultured after day 8 |
| • Samples with CT values 13–17 all led to positive culture | ||
| • No virus was successfully cultured when Ct values were ≥34 | ||
| Million et al. [46] (France) | 11 hospitalized PCR-positive patients in whom daily cultures were attempted past 10 days | • Virus unable to be cultured after day 10 |
| Bullard et al. [47] (Canada) | 90 PCR-positive nasopharyngeal or endotracheal aspirate samples taken through day 21 after symptom onset (unknown number of patients and severity of illness) | • Virus unable to be cultured after day 8 from symptom onset, or when Ct values were >24 |
| • Probability of culturing virus highest between days one and five and peaked on day 3 | ||
| • Each 1 unit increase in Ct value correlated with 32% decrease in odds of culturing virus | ||
| Liu et al. [25] (Taiwan) | 1 PCR-positive patient with mild febrile illness | • PCR positive through day 63 after symptom onset, but virus unable to be cultured after 18 days |
| van Kampen et al. [48] (Netherlands) | 690 upper and lower respiratory samples taken from 129 hospitalized patients with severe or critical illness, including 30 immunosuppresed patients | • Median duration of infectious shedding by viral culture = 8 days after symptom onset (IQR 5–11 days, maximum 20 days) |
| • Probability of obtaining infectious virus fell to <5% after 15 days from symptom onset | ||
| • Detection of viral RNA by PCR exceeded detection by culture | ||
| Cheng et al. [49] (Taiwan) | 100 patients with Covid-19 (mostly mild disease) | • Amongst 2761 close contacts, secondary attack rate was 0.7% amongst 1818 people who had contact within 5 days of symptom onset and 0% amongst 852 people who had contact ≥6 days after symptom onset |
| Lu et al. [50] (China) | 87 patients hospitalized patients with Covid-19, discharged after recovery and 2 consecutive negative PCR swabs, and then tested positive again within 2 weeks | • Viral cell culture and full-length genome sequencing unsuccessful in all cases |
| Korean Centers for Disease Control and Prevention [51] (South Korea) | 285 patients who recovered from Covid-19, tested negative, and then tested postive again by PCR (on average 45 days after initial symptom onset) | • Viral cell culture negative in 108 cases |
| • Ct values for re-postive tests >30 in 89.5% of cases | ||
| • 0% transmission to 790 contacts during re-positive period |
Summary of Studies Assessing Duration of SARS-CoV-2 Infectivity Based on Viral Cell Culture or Secondary Infection Rates
| Study (Country) | Population | Primary findings |
|---|---|---|
| Wolfel et al. [6] (Germany) | 9 young to middle-aged patients with mild disease | • Peak viral load prior to day 5 after symptom onset |
| • Virus unable to be cultured after day 8 from respiratory samples despite ongoing high viral load | ||
| • Virus unable to be cultured from stool, even with high viral load | ||
| U.S. Centers for Disease Control and Prevention [43] (U.S.) | Per CDC, data generated from adults across a variety of age groups and with varying severity of illness (unspecified number of patients) | • Virus unable to be cultured more than 9 days after symptom onset |
| • Attempts to culture virus from upper respiratory specimens largely unsuccessful when Ct values >33–35 | ||
| • Among patients who continue to have detectable RNA in upper respiratory specimens following clincal illness, concentrations are generally in the range at which replication-competent virus has not been reliably isolated | ||
| Young et al. [44] Singapore | 100 hospitalized patients (20 requiring supplemental oxygen and 12 requiring mechanical ventilation | • Viral culture unsuccessful in all PCR-positive samples with Ct values >30 |
| • 90% of all samples taken after day 14 from symptom onset had Ct values >30 | ||
| La Scola et al. [45] (France) | 183 PCR-positive samples (174 nasopharyngeal, 9 sputum) from 155 patients (unknown severity of illness) | • PCR tests positive for up to 20 days after symptom onset, but virus unable to be cultured after day 8 |
| • Samples with CT values 13–17 all led to positive culture | ||
| • No virus was successfully cultured when Ct values were ≥34 | ||
| Million et al. [46] (France) | 11 hospitalized PCR-positive patients in whom daily cultures were attempted past 10 days | • Virus unable to be cultured after day 10 |
| Bullard et al. [47] (Canada) | 90 PCR-positive nasopharyngeal or endotracheal aspirate samples taken through day 21 after symptom onset (unknown number of patients and severity of illness) | • Virus unable to be cultured after day 8 from symptom onset, or when Ct values were >24 |
| • Probability of culturing virus highest between days one and five and peaked on day 3 | ||
| • Each 1 unit increase in Ct value correlated with 32% decrease in odds of culturing virus | ||
| Liu et al. [25] (Taiwan) | 1 PCR-positive patient with mild febrile illness | • PCR positive through day 63 after symptom onset, but virus unable to be cultured after 18 days |
| van Kampen et al. [48] (Netherlands) | 690 upper and lower respiratory samples taken from 129 hospitalized patients with severe or critical illness, including 30 immunosuppresed patients | • Median duration of infectious shedding by viral culture = 8 days after symptom onset (IQR 5–11 days, maximum 20 days) |
| • Probability of obtaining infectious virus fell to <5% after 15 days from symptom onset | ||
| • Detection of viral RNA by PCR exceeded detection by culture | ||
| Cheng et al. [49] (Taiwan) | 100 patients with Covid-19 (mostly mild disease) | • Amongst 2761 close contacts, secondary attack rate was 0.7% amongst 1818 people who had contact within 5 days of symptom onset and 0% amongst 852 people who had contact ≥6 days after symptom onset |
| Lu et al. [50] (China) | 87 patients hospitalized patients with Covid-19, discharged after recovery and 2 consecutive negative PCR swabs, and then tested positive again within 2 weeks | • Viral cell culture and full-length genome sequencing unsuccessful in all cases |
| Korean Centers for Disease Control and Prevention [51] (South Korea) | 285 patients who recovered from Covid-19, tested negative, and then tested postive again by PCR (on average 45 days after initial symptom onset) | • Viral cell culture negative in 108 cases |
| • Ct values for re-postive tests >30 in 89.5% of cases | ||
| • 0% transmission to 790 contacts during re-positive period |
| Study (Country) | Population | Primary findings |
|---|---|---|
| Wolfel et al. [6] (Germany) | 9 young to middle-aged patients with mild disease | • Peak viral load prior to day 5 after symptom onset |
| • Virus unable to be cultured after day 8 from respiratory samples despite ongoing high viral load | ||
| • Virus unable to be cultured from stool, even with high viral load | ||
| U.S. Centers for Disease Control and Prevention [43] (U.S.) | Per CDC, data generated from adults across a variety of age groups and with varying severity of illness (unspecified number of patients) | • Virus unable to be cultured more than 9 days after symptom onset |
| • Attempts to culture virus from upper respiratory specimens largely unsuccessful when Ct values >33–35 | ||
| • Among patients who continue to have detectable RNA in upper respiratory specimens following clincal illness, concentrations are generally in the range at which replication-competent virus has not been reliably isolated | ||
| Young et al. [44] Singapore | 100 hospitalized patients (20 requiring supplemental oxygen and 12 requiring mechanical ventilation | • Viral culture unsuccessful in all PCR-positive samples with Ct values >30 |
| • 90% of all samples taken after day 14 from symptom onset had Ct values >30 | ||
| La Scola et al. [45] (France) | 183 PCR-positive samples (174 nasopharyngeal, 9 sputum) from 155 patients (unknown severity of illness) | • PCR tests positive for up to 20 days after symptom onset, but virus unable to be cultured after day 8 |
| • Samples with CT values 13–17 all led to positive culture | ||
| • No virus was successfully cultured when Ct values were ≥34 | ||
| Million et al. [46] (France) | 11 hospitalized PCR-positive patients in whom daily cultures were attempted past 10 days | • Virus unable to be cultured after day 10 |
| Bullard et al. [47] (Canada) | 90 PCR-positive nasopharyngeal or endotracheal aspirate samples taken through day 21 after symptom onset (unknown number of patients and severity of illness) | • Virus unable to be cultured after day 8 from symptom onset, or when Ct values were >24 |
| • Probability of culturing virus highest between days one and five and peaked on day 3 | ||
| • Each 1 unit increase in Ct value correlated with 32% decrease in odds of culturing virus | ||
| Liu et al. [25] (Taiwan) | 1 PCR-positive patient with mild febrile illness | • PCR positive through day 63 after symptom onset, but virus unable to be cultured after 18 days |
| van Kampen et al. [48] (Netherlands) | 690 upper and lower respiratory samples taken from 129 hospitalized patients with severe or critical illness, including 30 immunosuppresed patients | • Median duration of infectious shedding by viral culture = 8 days after symptom onset (IQR 5–11 days, maximum 20 days) |
| • Probability of obtaining infectious virus fell to <5% after 15 days from symptom onset | ||
| • Detection of viral RNA by PCR exceeded detection by culture | ||
| Cheng et al. [49] (Taiwan) | 100 patients with Covid-19 (mostly mild disease) | • Amongst 2761 close contacts, secondary attack rate was 0.7% amongst 1818 people who had contact within 5 days of symptom onset and 0% amongst 852 people who had contact ≥6 days after symptom onset |
| Lu et al. [50] (China) | 87 patients hospitalized patients with Covid-19, discharged after recovery and 2 consecutive negative PCR swabs, and then tested positive again within 2 weeks | • Viral cell culture and full-length genome sequencing unsuccessful in all cases |
| Korean Centers for Disease Control and Prevention [51] (South Korea) | 285 patients who recovered from Covid-19, tested negative, and then tested postive again by PCR (on average 45 days after initial symptom onset) | • Viral cell culture negative in 108 cases |
| • Ct values for re-postive tests >30 in 89.5% of cases | ||
| • 0% transmission to 790 contacts during re-positive period |
Likewise, the US CDC reported they have not been able to isolate culture replication-competent virus from patients >9 days from symptom onset [43]. These data were generated from adult patients spanning a range of ages and severities of illness, although CDC did not specify the number of patients in their analysis. Attempts to culture virus from upper respiratory specimens were unsuccessful when PCR Ct values were higher than 35 (ie, a low but detectable range of viral nucleic acid). Ct values from upper respiratory specimens were high following recovery from clinical illness, suggesting viral debris rather than replication-competent virus. Lastly, the CDC reported that they have not cultured infectious virus from urine or from feces, suggesting these sources pose minimal risk of transmission, particularly following hand hygiene. Note, however, that investigators have been able to culture infectious virus from feces in at least one patient [52].
Similar results were reported in two studies from Southern France that retrospectively examined the effect of hydroxychloroquine and azithromycin on clinical and virologic outcomes [45, 46]. In the first analysis, 183 PCR-positive samples (including 174 nasopharyngeal swabs and 9 sputum) from 155 patients were inoculated in cell cultures, of which 129 led to successful isolation [45]. Samples with Ct values of 13–17 were all associated with positive viral cultures. The culture positivity rate steadily decreased with rising Ct values, and no virus was successfully cultured from samples with Ct values ≥34. PCR tests were positive for up to 20 days after symptom onset, but viable virus could not be cultured after day 8. In the second analysis, 11 patients in whom daily cultures were attempted were negative by day 10 [46].
Canadian investigators provided similar results from an analysis of 90 PCR-positive samples, including nasopharyngeal swabs and endotracheal aspirates, taken through 21 days after symptom onset [47]. Virus could not be cultured after 8 days from symptom onset or when Ct values were greater than 24. The probability of successfully culturing SARS-CoV-2 was highest between days 1–5 and peaked at day 3. Every unit increase in Ct value was associated with a decrease in the odds of successfully culturing virus by 32%.
In an analysis of hospitalized patients with Covid-19 in Singapore, viral culture was positive from respiratory samples in 14 of 73 patients [44]. Viral culture was unsuccessful in all samples with Ct values >30, and 90% of samples taken after day 14 from symptom onset had Ct values >30.
A study from the Netherlands specifically focused on patients with severe illness, including immunocompromised patients [48]. Of the 129 patients in the study, 69% were in intensive care units, 31% were in noncritical care units (most of whom required supplemental oxygen), 23% and were immunosuppressed. The investigators tested 690 upper and lower respiratory samples at various time points for viable virus using cell culture; 23 of the 129 patients (17.8%) had replication-competent virus. The median interval of infectious shedding by culture was 8 days after symptom onset (interquartile range 5–11). The maximum interval from symptom onset associated with viable virus was 20 days (occurring in one patient); unfortunately, the clinical characteristics and illness trajectory of this patient were not reported. The median viral load was significantly higher in culture-positive samples than culture-negative samples, and the probability of detecting replication-competent virus was <5% after 15 days from symptom onset.
Although the duration of infectivity is generally longer in severe illness, outliers may be possible. One case report from Taiwan, for example, noted infectious shedding by viral cell culture in the sputum 18 days after symptom onset in a patient with a mild febrile illness [53]. In addition, effective antiviral therapy is associated with a shorter time to negative SARS-CoV-2 viral load, although its impact on transmissibility has not yet been established [54].
EPIDEMIOLOGICAL DATA on TRANSMISSIBILITY
The data on duration of viral recovery in cell culture following symptom onset are mirrored by data on transmission rates. In a prospective study conducted in Taiwan, 100 confirmed Covid-19 cases and their contacts were identified and the secondary clinical attack rate was measured for different time intervals from symptom-onset [49]. There were 2761 close contacts of the 100 cases; the secondary attack rate was 0.7% amongst the 1818 people with contact with case patients within 5 days of symptom onset and 0% amongst the 852 people with contact >5 days after symptom onset. As with other studies, attack rates were highest among household and family contacts (~5%) and substantially lower amongst healthcare contacts (0.9%). Notably, though, only 6 of the confirmed index cases had severe disease; the 786 close contacts of these severely ill patients were about 4 times more likely to acquire infection compared to the 1097 close contacts of 56 patients with mild disease.
SIGNIFICANCE of PATIENTS WHO TEST PCR-POSITIVE AFTER TESTING NEGATIVE
Investigators from Guangdong Province, China, analyzed 619 hospitalized patients with Covid-19 who were discharged after resolution of fever, improvement in respiratory symptoms, and 2 consecutive negative PCR samples >24 h apart on both respiratory tract and gastrointestinal tract samples [50]. All discharged cases were isolated in designated hotels, kept in observation, and retested on days 7 and 14 after recovery. 87 patients (14.1%) tested positive, of whom 77 were asymptomatic and 10 had mild cough. Viral cell culture was unsuccessful in all cases; furthermore, full-length genomes could not be sequenced in any cases, suggesting genome degradation.
Similarly, the Korean CDC reported on epidemiologic and contact tracing for 285 patients who recovered from Covid-19, tested negative, and then tested positive again by PCR [51]. On average, the re-positive test occurred 45 days after initial symptom onset (range 8–82 days). Retesting was done in 37.5% of patients because of new symptoms such as cough or sore throat. Viral cell culture testing was done in 108 re-positive cases, and all were negative. PCR Ct values were >30 in 89.5% of cases, suggesting that the negative-to-positive phenomenon represents sampling variability near the assay limit of detection. None of 790 contacts of the 285 re-positive cases (including 351 family members) developed Covid-19.
DEGREE AND DURATION OF IMMUNITY FOLLOWING INFECTION
An important question is to what degree individuals who have recovered from Covid-19 are vulnerable to SARS-CoV-2 re-infection and how long immunity might last. Animal studies demonstrate that infection provides at least short-term immunity. One group of investigators experimentally infected 9 rhesus macaques with SARS-CoV-2, after which all developed neutralizing antibodies [55]. When the monkeys were re-challenged with the same viral dose 35 days later, all demonstrated anamnestic immune responses, with lower nasal viral RNA levels and more rapid declines in viral RNA compared to the initial challenge and compared to control monkeys. A separate study conducted in China using 7 rhesus macaque monkeys demonstrated similar findings [56]. Monkeys were infected and underwent a mild-to-moderate course of disease. Four of the seven macaques were re-challenged 28 days later; none showed any clinical signs of disease, viral dissemination, or histopathological changes on necropsy.
In humans, several cases of re-infection with SARS-CoV-2 have now been confirmed using whole genome sequencing. Although the true incidence of re-infection shortly after an initial infection is unknown, it is likely rare. As described above, most obsolete reports of recurrent positive PCR tests likely reflect residual RNA with high Ct values. Small case series in humans also suggest that neutralizing antibodies develop in most patients following recovery from Covid-19, and that titers correlate with severity of illness and the number of virus-specific T-cells [5, 6, 57–60]. However, in one study of 74 patients with symptomatic and asymptomatic infection, most demonstrated a decrease in IgG levels and neutralizing antibodies within 2–3 months after infection; 40% of asymptomatic individuals became seronegative in the early convalescent phase, compared to 12.9% of symptomatic patients [61]. Another study demonstrated an IgG half-life of 73 days in patients with mild illness [62]. It is unclear, however, whether and to what extent the decrease in measurable antibody levels correlates with loss of functional immunity.
SUMMARY AND IMPLICATIONS FOR PUBLIC HEALTH RECOMMENDATIONS
In summary, based on a rapidly expanding evidence base, we currently draw the following conclusions regarding the timing and duration of SARS-CoV-2 transmissibility (Figure 1):
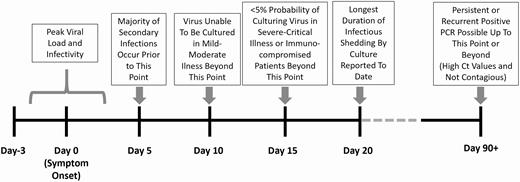
Summary of timeline of SARS-CoV-2 infectivity.
SARS-CoV-2 is most contagious right before and immediately following symptom onset.
Contagiousness rapidly decreases to near-zero after about 10 days from symptom onset in mild-moderately ill patients and 15 days in critically ill and immunocompromised patients. The longest duration of viral viability that has been reported thus far is 20 days from symptom onset.
Persistently positive SARS-CoV-2 RNA PCRs in recovered patients are common but are generally associated with high Ct values, reflecting low viral loads. These do not indicate replication-competent virus and are not associated with contagiousness.
PCR assays that alternate between positive and negative results in patients who have recovered from Covid-19 most likely reflect sampling variability and low levels of viral debris at the borderline of detection. These patients are unlikely to be contagious.
Infection confers at least short-term immunity in most cases; however, the duration of immunity is unclear and several cases of re-infection have now been confirmed.
These data have informed evolving national and international public health recommendations (Table 2). WHO, for example, initially recommended 2 negative PCR results on sequential samples taken >24 h apart in clinically recovered patients before discontinuing isolation. On May 27, WHO shifted to recommending isolation for 10 days after symptom onset, plus at least 3 additional days without symptoms [63]. In asymptomatic patients, WHO recommends discontinuing isolation 10 days after the positive PCR test. WHO still allows providers the option of using serial negative tests to clear patients but acknowledges that some patients have prolonged viral RNA detection by PCR that does not correlate with infectivity.
WHO and CDC Guidance for Discontinuing Isolation in Patients with Confirmed Covid-19 Infection and Approach to Persistent or Recurrent Positive PCR Tests
| Category | WHO | CDC |
|---|---|---|
| Symptomatic, initial infection | • 10 days after symptom onset, plus | • Mild-moderate Illness, Not Severely Immunocompromised: 10 days since symptom onset + 24 h since last fever + improvement in symptoms |
| • At least 3 additional days without symptoms (fever or respiratory symptoms) | ||
| • Severe-critical Illness OR Severely Immunocompromised: At least 10 days and up to 20 days since symptom onset + 24 h since last fever + improvement in symptoms | ||
| Asymptomatic, initial infection | • 10 days after positive test | • Not Severely Immunocompromised: 10 days since first positive test |
| • Severely Immunocompromised: At least 20 days and up to 20 days since first positive test | ||
| Recovered from Covid-19 but persistent or pecurrent PCR positive | • No specific recommendation | • Asymptomatic: Retesting not recommended within 3 months after date of symptom onset, even if the patient has close contact with an infected person. |
| • Symptomatic: If new symptoms develop within 3 months of initial symptom onset, and alternative etiology cannot be identified, consider retesting. Isolation may be considered in consultation with infectious disease or infection control experts, especially if symptoms developed within 14 days after close contact with an infected person. |
| Category | WHO | CDC |
|---|---|---|
| Symptomatic, initial infection | • 10 days after symptom onset, plus | • Mild-moderate Illness, Not Severely Immunocompromised: 10 days since symptom onset + 24 h since last fever + improvement in symptoms |
| • At least 3 additional days without symptoms (fever or respiratory symptoms) | ||
| • Severe-critical Illness OR Severely Immunocompromised: At least 10 days and up to 20 days since symptom onset + 24 h since last fever + improvement in symptoms | ||
| Asymptomatic, initial infection | • 10 days after positive test | • Not Severely Immunocompromised: 10 days since first positive test |
| • Severely Immunocompromised: At least 20 days and up to 20 days since first positive test | ||
| Recovered from Covid-19 but persistent or pecurrent PCR positive | • No specific recommendation | • Asymptomatic: Retesting not recommended within 3 months after date of symptom onset, even if the patient has close contact with an infected person. |
| • Symptomatic: If new symptoms develop within 3 months of initial symptom onset, and alternative etiology cannot be identified, consider retesting. Isolation may be considered in consultation with infectious disease or infection control experts, especially if symptoms developed within 14 days after close contact with an infected person. |
Note: WHO also allows for a test-based strategy to discontinue isolation based on clinical recovery and 2 sequential negative PCR tests >24 h apart. CDC no longer recommends a test-based strategy, except to discontinue isolation earlier than outlined by the time-based strategy, or possibly in persons who are severely immunocompromised (in consultation with infectious disease experts).
CDC definitions (severity of illness criteria adapted from the NIH COVID-19 Treatment Guidelines [https://www.covid19treatmentguidelines.nih.gov/overview/management-of-covid-19/]):
• Mild Illness: Individuals who have any of the various signs and symptoms of COVID-19 (eg, fever, cough, sore throat, malaise, headache, muscle pain) without shortness of breath, dyspnea, or abnormal chest imaging.
• Moderate Illness: Individuals who have evidence of lower respiratory disease by clinical assessment or imaging, and a saturation of oxygen (SpO2) ≥94% on room air at sea level.
• Severe Illness: Individuals who have respiratory frequency > 30 breaths per minute, SpO2 <94% on room air at sea level (or, for patients with chronic hypoxemia, a decrease from baseline of >3%), ratio of arterial partial pressure of oxygen to fraction of inspired oxygen (PaO2/FiO2) <300 mmHg, or lung infiltrates >50%
• Critical Illness: Individuals who have respiratory failure, septic shock, and/or multiple organ dysfunction.
• Severely Immunocompromised: chemotherapy for cancer, untreated HIV infection with CD4 T lymphocyte count <200, combined primary immunodeficiency disorder, and receipt of prednisone >20mg/day for more than 14 days.
WHO and CDC Guidance for Discontinuing Isolation in Patients with Confirmed Covid-19 Infection and Approach to Persistent or Recurrent Positive PCR Tests
| Category | WHO | CDC |
|---|---|---|
| Symptomatic, initial infection | • 10 days after symptom onset, plus | • Mild-moderate Illness, Not Severely Immunocompromised: 10 days since symptom onset + 24 h since last fever + improvement in symptoms |
| • At least 3 additional days without symptoms (fever or respiratory symptoms) | ||
| • Severe-critical Illness OR Severely Immunocompromised: At least 10 days and up to 20 days since symptom onset + 24 h since last fever + improvement in symptoms | ||
| Asymptomatic, initial infection | • 10 days after positive test | • Not Severely Immunocompromised: 10 days since first positive test |
| • Severely Immunocompromised: At least 20 days and up to 20 days since first positive test | ||
| Recovered from Covid-19 but persistent or pecurrent PCR positive | • No specific recommendation | • Asymptomatic: Retesting not recommended within 3 months after date of symptom onset, even if the patient has close contact with an infected person. |
| • Symptomatic: If new symptoms develop within 3 months of initial symptom onset, and alternative etiology cannot be identified, consider retesting. Isolation may be considered in consultation with infectious disease or infection control experts, especially if symptoms developed within 14 days after close contact with an infected person. |
| Category | WHO | CDC |
|---|---|---|
| Symptomatic, initial infection | • 10 days after symptom onset, plus | • Mild-moderate Illness, Not Severely Immunocompromised: 10 days since symptom onset + 24 h since last fever + improvement in symptoms |
| • At least 3 additional days without symptoms (fever or respiratory symptoms) | ||
| • Severe-critical Illness OR Severely Immunocompromised: At least 10 days and up to 20 days since symptom onset + 24 h since last fever + improvement in symptoms | ||
| Asymptomatic, initial infection | • 10 days after positive test | • Not Severely Immunocompromised: 10 days since first positive test |
| • Severely Immunocompromised: At least 20 days and up to 20 days since first positive test | ||
| Recovered from Covid-19 but persistent or pecurrent PCR positive | • No specific recommendation | • Asymptomatic: Retesting not recommended within 3 months after date of symptom onset, even if the patient has close contact with an infected person. |
| • Symptomatic: If new symptoms develop within 3 months of initial symptom onset, and alternative etiology cannot be identified, consider retesting. Isolation may be considered in consultation with infectious disease or infection control experts, especially if symptoms developed within 14 days after close contact with an infected person. |
Note: WHO also allows for a test-based strategy to discontinue isolation based on clinical recovery and 2 sequential negative PCR tests >24 h apart. CDC no longer recommends a test-based strategy, except to discontinue isolation earlier than outlined by the time-based strategy, or possibly in persons who are severely immunocompromised (in consultation with infectious disease experts).
CDC definitions (severity of illness criteria adapted from the NIH COVID-19 Treatment Guidelines [https://www.covid19treatmentguidelines.nih.gov/overview/management-of-covid-19/]):
• Mild Illness: Individuals who have any of the various signs and symptoms of COVID-19 (eg, fever, cough, sore throat, malaise, headache, muscle pain) without shortness of breath, dyspnea, or abnormal chest imaging.
• Moderate Illness: Individuals who have evidence of lower respiratory disease by clinical assessment or imaging, and a saturation of oxygen (SpO2) ≥94% on room air at sea level.
• Severe Illness: Individuals who have respiratory frequency > 30 breaths per minute, SpO2 <94% on room air at sea level (or, for patients with chronic hypoxemia, a decrease from baseline of >3%), ratio of arterial partial pressure of oxygen to fraction of inspired oxygen (PaO2/FiO2) <300 mmHg, or lung infiltrates >50%
• Critical Illness: Individuals who have respiratory failure, septic shock, and/or multiple organ dysfunction.
• Severely Immunocompromised: chemotherapy for cancer, untreated HIV infection with CD4 T lymphocyte count <200, combined primary immunodeficiency disorder, and receipt of prednisone >20mg/day for more than 14 days.
In July and August, CDC modified their guidance to a more nuanced approach based on severity-of-illness and immunocompetence [64]. Specifically, while CDC still recommends 10 days of isolation from symptom onset (including >24 h since resolution of fever and improvement in symptoms) for mild-moderately ill patients without severely immunocompromising conditions, they now recommend at least 10 days and up to 20 days for patients with severe-critical illness or severely immunocompromising conditions. For asymptomatic patients, 10 days is recommended from the first positive PCR test (and up to 20 days for severely immunocompromised patients). Moreover, CDC recommends avoiding test-based clearance given the evidence that people with persistently positive PCR tests are not contagious. Test-based clearance should be reserved for rare cases when there is a need to discontinue isolation early, or potentially to inform a decision to prolong isolation for severely immunocompromised patients.
ROLE OF PCR TESTING AFTER CLINICAL RECOVERY
CDC now recommends that patients who have recovered from Covid-19 and remain asymptomatic should not be retested within 3 months after symptom onset, even if they had close contact with another infected person [43]. This is based on observations that persons infected with related endemic human betacoronaviruses become susceptible to reinfection after about 90 days, and therefore a positive SARS-CoV-2 PCR test within 90 days of an initial infection most likely represents persistent viral debris rather than reinfection. For new symptoms potentially consistent with COVID-19 that develop within 3 months and are not clearly attributable to another diagnosis (such as influenza), CDC states that isolation may be warranted while evaluating for possible SARS-CoV-2 reinfection, in consultation with an infectious disease or infection control expert.
The optimal approach for isolating asymptomatic patients who test positive again >90 days from the original infection (for example, as part of a contact tracing investigation, or during routine screening upon admission to a healthcare facility) remains uncertain. This phenomenon, in our experience, is not uncommon, and most of these patients have high PCR Ct values suggestive of residual viral debris. We believe that the decision to isolate should be made on a case-by-case basis in consultation with infectious disease/infection control experts and/or local public health authorities, taking into account the patient’s medical history, time from initial positive test, PCR Ct value, and immune status. Given the uncertainty regarding duration of immunity and reports of confirmed SARS-CoV-2 re-infection in some patients, we believe it is prudent at this time to test all recovered patients who develop new symptoms > 3 months after initial infection and to isolate them if the PCR test is positive.
Conclusions
Much progress has been made in understanding the transmission dynamics of SARS-CoV-2 and duration of infectivity. WHO and CDC have modified their recommendations in response to data indicating that infectivity decreases to essentially zero after about 10 days from symptom onset in mild-moderately ill patients and after about 15 days in critically ill and immunocompromised patients, with a maximum reported interval thus far of 20 days. Additional data confirming these findings in larger and more diverse cohorts are needed to provide further reassurance as to the safety of discontinuing isolation for critically ill, deeply immunocompromised, and otherwise high-risk patients, and to define the optimal approach to retesting and isolation in patients who have recovered from Covid-19.
Notes
Role of the funder. The Centers for Disease Control and Prevention and Agency for Healthcare Research and Quality had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Financial support. This work was funded by the Centers for Disease Control and Prevention (6U54CK000484-04-02) and the Agency for Healthcare Research and Quality (K08HS025008 to C.R.).
Potential conflicts of interest. M. K. and C. R. report personal fees from UpToDate, outside the submitted work. All other authors have no potential conflicts to disclose. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.


{kind=link}
Comments