





Preamble
Guidelines and Expert Consensus documents aim to present all the relevant evidence on a particular issue in order to help physicians to weigh the benefits and risks of a particular diagnostic or therapeutic procedure. They should be helpful in everyday clinical decision-making.
A great number of Guidelines and Expert Consensus Documents have been issued in recent years by different organisations, the European Society of Cardiology (ESC) and by other related societies. By means of links to web sites of National Societies several hundred guidelines are available. This profusion can put at stake the authority and validity of guidelines, which can only be guaranteed if they have been developed by an unquestionable decision-making process. This is one of the reasons why the ESC and others have issued recommendations for formulating and issuing Guidelines and Expert Consensus Documents.
In spite of the fact that standards for issuing good quality Guidelines and Expert Consensus Documents are well defined, recent surveys of Guidelines and Expert Consensus Documents published in peer-reviewed journals between 1985 and 1998 have shown that methodological standards were not complied within the vast majority of cases. It is therefore of great importance that guidelines and recommendations are presented in formats that are easily interpreted. Subsequently, their implementation programmes must also be well conducted. Attempts have been made to determine whether guidelines improve the quality of clinical practice and the utilisation of health resources.
The ESC Committee for Practice Guidelines (CPG) supervises and coordinates the preparation of new Guidelines and Expert Consensus Documents produced by Task Forces, expert groups or consensus panels. The Committee is also responsible for the endorsement of these Guidelines and Expert Consensus Documents or statements.
Introduction
The strength of evidence related to a particular diagnostic or treatment option depends on the available data: (1) level of evidence A: multiple randomised clinical trials or meta-analyses; (2) level of evidence B: a single randomised trial or non-randomised studies; and (3) level of evidence C: consensus opinion of the experts. Indications for various tests and procedures were ranked in three classes:
Conditions for which there is evidence and/or general agreement that a given procedure or treatment is useful and effective.
Conditions for which there is conflicting evidence and/or a divergence of opinion about the usefulness/efficacy of a procedure or treatment.
Weight of evidence/opinion is in favour of usefulness/efficacy.
Usefulness/efficacy is less well established by evidence/opinion.
Conditions for which there is evidence and/or general agreement that the procedure/treatment is not useful/effective and in some cases may be harmful.
Aetiology and classification of pericardial disease
The spectrum of pericardial diseases consists of congenital defects, pericarditis (dry, effusive, effusive-constrictive, and constrictive), neoplasm, and cysts. The aetiological classification comprises: infectious pericarditis, pericarditis in systemic autoimmune diseases, type 2 (auto) immune process, postmyocardial infarction syndrome, and auto-reactive (chronic) pericarditis (Table 1).1–3
Review of aetiology, incidence and pathogenesis of pericarditis1–3
Aetiology | Incidence (%) | Pathogenesis | ||
|---|---|---|---|---|
| Infectious pericarditis | Multiplication and spread of the causative agent and release of toxic substances in pericardial tissue cause serous, serofibrinous or haemorrhagic (bacterial, viral, tuberculous, fungal) or purulent inflammation (bacterial) | |||
| Viral (Coxsackie A9, B1-4, Echo 8, Mumps, EBV, CMV, Varicella, Rubella, HIV, Parvo B19, etc.) | 30–50a | |||
| Bacterial (Pneumo-, Meningo-, Gonococcosis, Hemophilus, Treponema pallidum, Borreliosis, Chlamydia, Tuberculosis, etc.) | 5–10a | |||
| Fungal (Candida, Histoplasma, etc.) | Rare | |||
| Parasitary (Entameba histolytica, Echinococcus, Toxoplasma…) | Rare | |||
| Pericarditis in systemic autoimmune diseases | Cardiac manifestations of the basic disease, often clinically mild or silent | |||
| Systemic lupus erythematosus | 30b | |||
| Rheumatoid arthritis | 30b | |||
| Spondylitis ankylosans | 1b | |||
| Systemic sclerosis | \(>\) 50b | |||
| Dermatomyositis | Rare | |||
| Periarteritis nodosa | Rare | |||
| Reiter's syndrome | ∼2b | |||
| Familial Mediterranean fever | 0.7b | |||
| Type 2 (auto)immune process | Secondary, after infection/surgery | |||
| Rheumatic fever | 20–50b | Mostly in acute phase | ||
| Postcardiotomy syndrome | ∼20b | 10–14 days after surgery | ||
| Postmyocardial infarction syndrome | 1–5b | DDg P. epistenocardica | ||
| Autoreactive (chronic) pericarditis | 23.1a | Common form | ||
| Pericarditis and pericardial effusion in diseases of surrounding organs | ||||
| Acute MI (P. epistenocardica) | 5–20b | 1–5 days after transmural MI | ||
| Myocarditis | 30b | Accompanying epimyocarditis | ||
| Aortic aneurysm | Rare | Dissection: haemorrhagic PE | ||
| Lung infarction | Rare | |||
| Pneumonia | Rare | |||
| Oesophageal diseases | Rare | |||
| Hydropericardium in CHF | Rare | |||
| Paraneoplastic pericarditis | Frequent | No direct neoplastic infiltrate | ||
| Pericarditis in metabolic disorders | ||||
| Renal insufficiency (uraemia) | Frequent | Viral/toxic/autoimmune | ||
| Myxedema | 30b | Serous, cholesterol rich PE | ||
| Addison's disease | Rare | Membranous leak? | ||
| Diabetic ketoacidosis | Rare | |||
| Cholesterol pericarditis | Very rare | Transudation of cholesterol (sterile serofibrinous PE) | ||
| Pregnancy | Rare | |||
| Traumatic pericarditis | ||||
| Direct injury (penetrating thoracic injury, oesophageal perforation, foreign bodies) | Rare | |||
| Indirect injury (Non-penetrating thoracic injury, mediastinal irradiation) | Rare | Less frequent after introduction of topical convergent irradiation | ||
| Neoplastic pericardial disease | 35a | |||
| Primary tumours | Rare | |||
| Secondary metastatic tumours | Frequent | |||
| Lung carcinoma | 40c | Serous or fibrinous, frequently haemorrhagic effusion | ||
| Breast carcinoma | 22c | Accompanying disease during the infiltration of malignant cells | ||
| Gastric and colon | 3c | |||
| Other carcinoma | 6c | |||
| Leukemia and lymphoma | 15c | |||
| Melanoma | 3c | |||
| Sarcoma | 4c | |||
| Other tumours | 7c | |||
| Idiopathic | 3.5a, in other series \(>\) 50a | Serous, fibrinous, sometimes haemorrhagic PE with suspect viral or autoimmune secondary immunopathogenesis | ||
Aetiology | Incidence (%) | Pathogenesis | ||
|---|---|---|---|---|
| Infectious pericarditis | Multiplication and spread of the causative agent and release of toxic substances in pericardial tissue cause serous, serofibrinous or haemorrhagic (bacterial, viral, tuberculous, fungal) or purulent inflammation (bacterial) | |||
| Viral (Coxsackie A9, B1-4, Echo 8, Mumps, EBV, CMV, Varicella, Rubella, HIV, Parvo B19, etc.) | 30–50a | |||
| Bacterial (Pneumo-, Meningo-, Gonococcosis, Hemophilus, Treponema pallidum, Borreliosis, Chlamydia, Tuberculosis, etc.) | 5–10a | |||
| Fungal (Candida, Histoplasma, etc.) | Rare | |||
| Parasitary (Entameba histolytica, Echinococcus, Toxoplasma…) | Rare | |||
| Pericarditis in systemic autoimmune diseases | Cardiac manifestations of the basic disease, often clinically mild or silent | |||
| Systemic lupus erythematosus | 30b | |||
| Rheumatoid arthritis | 30b | |||
| Spondylitis ankylosans | 1b | |||
| Systemic sclerosis | \(>\) 50b | |||
| Dermatomyositis | Rare | |||
| Periarteritis nodosa | Rare | |||
| Reiter's syndrome | ∼2b | |||
| Familial Mediterranean fever | 0.7b | |||
| Type 2 (auto)immune process | Secondary, after infection/surgery | |||
| Rheumatic fever | 20–50b | Mostly in acute phase | ||
| Postcardiotomy syndrome | ∼20b | 10–14 days after surgery | ||
| Postmyocardial infarction syndrome | 1–5b | DDg P. epistenocardica | ||
| Autoreactive (chronic) pericarditis | 23.1a | Common form | ||
| Pericarditis and pericardial effusion in diseases of surrounding organs | ||||
| Acute MI (P. epistenocardica) | 5–20b | 1–5 days after transmural MI | ||
| Myocarditis | 30b | Accompanying epimyocarditis | ||
| Aortic aneurysm | Rare | Dissection: haemorrhagic PE | ||
| Lung infarction | Rare | |||
| Pneumonia | Rare | |||
| Oesophageal diseases | Rare | |||
| Hydropericardium in CHF | Rare | |||
| Paraneoplastic pericarditis | Frequent | No direct neoplastic infiltrate | ||
| Pericarditis in metabolic disorders | ||||
| Renal insufficiency (uraemia) | Frequent | Viral/toxic/autoimmune | ||
| Myxedema | 30b | Serous, cholesterol rich PE | ||
| Addison's disease | Rare | Membranous leak? | ||
| Diabetic ketoacidosis | Rare | |||
| Cholesterol pericarditis | Very rare | Transudation of cholesterol (sterile serofibrinous PE) | ||
| Pregnancy | Rare | |||
| Traumatic pericarditis | ||||
| Direct injury (penetrating thoracic injury, oesophageal perforation, foreign bodies) | Rare | |||
| Indirect injury (Non-penetrating thoracic injury, mediastinal irradiation) | Rare | Less frequent after introduction of topical convergent irradiation | ||
| Neoplastic pericardial disease | 35a | |||
| Primary tumours | Rare | |||
| Secondary metastatic tumours | Frequent | |||
| Lung carcinoma | 40c | Serous or fibrinous, frequently haemorrhagic effusion | ||
| Breast carcinoma | 22c | Accompanying disease during the infiltration of malignant cells | ||
| Gastric and colon | 3c | |||
| Other carcinoma | 6c | |||
| Leukemia and lymphoma | 15c | |||
| Melanoma | 3c | |||
| Sarcoma | 4c | |||
| Other tumours | 7c | |||
| Idiopathic | 3.5a, in other series \(>\) 50a | Serous, fibrinous, sometimes haemorrhagic PE with suspect viral or autoimmune secondary immunopathogenesis | ||
CHF, congestive heart failure; DDg, differential diagnosis; MI, myocardial infarction; P., pericarditis; PE, pericardial effusion.
Percentage related to the population of 260 subsequent patients undergoing pericardiocentesis, pericardioscopy and epicardial biopsy (Marburg pericarditis registry 1988–2001).1
Percentage related to the incidence of pericarditis in the specific population of patients (e.g., with systemic lupus erythematosus).
Percentage related to the population of patients with neoplastic pericarditis.
Review of aetiology, incidence and pathogenesis of pericarditis1–3
Aetiology | Incidence (%) | Pathogenesis | ||
|---|---|---|---|---|
| Infectious pericarditis | Multiplication and spread of the causative agent and release of toxic substances in pericardial tissue cause serous, serofibrinous or haemorrhagic (bacterial, viral, tuberculous, fungal) or purulent inflammation (bacterial) | |||
| Viral (Coxsackie A9, B1-4, Echo 8, Mumps, EBV, CMV, Varicella, Rubella, HIV, Parvo B19, etc.) | 30–50a | |||
| Bacterial (Pneumo-, Meningo-, Gonococcosis, Hemophilus, Treponema pallidum, Borreliosis, Chlamydia, Tuberculosis, etc.) | 5–10a | |||
| Fungal (Candida, Histoplasma, etc.) | Rare | |||
| Parasitary (Entameba histolytica, Echinococcus, Toxoplasma…) | Rare | |||
| Pericarditis in systemic autoimmune diseases | Cardiac manifestations of the basic disease, often clinically mild or silent | |||
| Systemic lupus erythematosus | 30b | |||
| Rheumatoid arthritis | 30b | |||
| Spondylitis ankylosans | 1b | |||
| Systemic sclerosis | \(>\) 50b | |||
| Dermatomyositis | Rare | |||
| Periarteritis nodosa | Rare | |||
| Reiter's syndrome | ∼2b | |||
| Familial Mediterranean fever | 0.7b | |||
| Type 2 (auto)immune process | Secondary, after infection/surgery | |||
| Rheumatic fever | 20–50b | Mostly in acute phase | ||
| Postcardiotomy syndrome | ∼20b | 10–14 days after surgery | ||
| Postmyocardial infarction syndrome | 1–5b | DDg P. epistenocardica | ||
| Autoreactive (chronic) pericarditis | 23.1a | Common form | ||
| Pericarditis and pericardial effusion in diseases of surrounding organs | ||||
| Acute MI (P. epistenocardica) | 5–20b | 1–5 days after transmural MI | ||
| Myocarditis | 30b | Accompanying epimyocarditis | ||
| Aortic aneurysm | Rare | Dissection: haemorrhagic PE | ||
| Lung infarction | Rare | |||
| Pneumonia | Rare | |||
| Oesophageal diseases | Rare | |||
| Hydropericardium in CHF | Rare | |||
| Paraneoplastic pericarditis | Frequent | No direct neoplastic infiltrate | ||
| Pericarditis in metabolic disorders | ||||
| Renal insufficiency (uraemia) | Frequent | Viral/toxic/autoimmune | ||
| Myxedema | 30b | Serous, cholesterol rich PE | ||
| Addison's disease | Rare | Membranous leak? | ||
| Diabetic ketoacidosis | Rare | |||
| Cholesterol pericarditis | Very rare | Transudation of cholesterol (sterile serofibrinous PE) | ||
| Pregnancy | Rare | |||
| Traumatic pericarditis | ||||
| Direct injury (penetrating thoracic injury, oesophageal perforation, foreign bodies) | Rare | |||
| Indirect injury (Non-penetrating thoracic injury, mediastinal irradiation) | Rare | Less frequent after introduction of topical convergent irradiation | ||
| Neoplastic pericardial disease | 35a | |||
| Primary tumours | Rare | |||
| Secondary metastatic tumours | Frequent | |||
| Lung carcinoma | 40c | Serous or fibrinous, frequently haemorrhagic effusion | ||
| Breast carcinoma | 22c | Accompanying disease during the infiltration of malignant cells | ||
| Gastric and colon | 3c | |||
| Other carcinoma | 6c | |||
| Leukemia and lymphoma | 15c | |||
| Melanoma | 3c | |||
| Sarcoma | 4c | |||
| Other tumours | 7c | |||
| Idiopathic | 3.5a, in other series \(>\) 50a | Serous, fibrinous, sometimes haemorrhagic PE with suspect viral or autoimmune secondary immunopathogenesis | ||
Aetiology | Incidence (%) | Pathogenesis | ||
|---|---|---|---|---|
| Infectious pericarditis | Multiplication and spread of the causative agent and release of toxic substances in pericardial tissue cause serous, serofibrinous or haemorrhagic (bacterial, viral, tuberculous, fungal) or purulent inflammation (bacterial) | |||
| Viral (Coxsackie A9, B1-4, Echo 8, Mumps, EBV, CMV, Varicella, Rubella, HIV, Parvo B19, etc.) | 30–50a | |||
| Bacterial (Pneumo-, Meningo-, Gonococcosis, Hemophilus, Treponema pallidum, Borreliosis, Chlamydia, Tuberculosis, etc.) | 5–10a | |||
| Fungal (Candida, Histoplasma, etc.) | Rare | |||
| Parasitary (Entameba histolytica, Echinococcus, Toxoplasma…) | Rare | |||
| Pericarditis in systemic autoimmune diseases | Cardiac manifestations of the basic disease, often clinically mild or silent | |||
| Systemic lupus erythematosus | 30b | |||
| Rheumatoid arthritis | 30b | |||
| Spondylitis ankylosans | 1b | |||
| Systemic sclerosis | \(>\) 50b | |||
| Dermatomyositis | Rare | |||
| Periarteritis nodosa | Rare | |||
| Reiter's syndrome | ∼2b | |||
| Familial Mediterranean fever | 0.7b | |||
| Type 2 (auto)immune process | Secondary, after infection/surgery | |||
| Rheumatic fever | 20–50b | Mostly in acute phase | ||
| Postcardiotomy syndrome | ∼20b | 10–14 days after surgery | ||
| Postmyocardial infarction syndrome | 1–5b | DDg P. epistenocardica | ||
| Autoreactive (chronic) pericarditis | 23.1a | Common form | ||
| Pericarditis and pericardial effusion in diseases of surrounding organs | ||||
| Acute MI (P. epistenocardica) | 5–20b | 1–5 days after transmural MI | ||
| Myocarditis | 30b | Accompanying epimyocarditis | ||
| Aortic aneurysm | Rare | Dissection: haemorrhagic PE | ||
| Lung infarction | Rare | |||
| Pneumonia | Rare | |||
| Oesophageal diseases | Rare | |||
| Hydropericardium in CHF | Rare | |||
| Paraneoplastic pericarditis | Frequent | No direct neoplastic infiltrate | ||
| Pericarditis in metabolic disorders | ||||
| Renal insufficiency (uraemia) | Frequent | Viral/toxic/autoimmune | ||
| Myxedema | 30b | Serous, cholesterol rich PE | ||
| Addison's disease | Rare | Membranous leak? | ||
| Diabetic ketoacidosis | Rare | |||
| Cholesterol pericarditis | Very rare | Transudation of cholesterol (sterile serofibrinous PE) | ||
| Pregnancy | Rare | |||
| Traumatic pericarditis | ||||
| Direct injury (penetrating thoracic injury, oesophageal perforation, foreign bodies) | Rare | |||
| Indirect injury (Non-penetrating thoracic injury, mediastinal irradiation) | Rare | Less frequent after introduction of topical convergent irradiation | ||
| Neoplastic pericardial disease | 35a | |||
| Primary tumours | Rare | |||
| Secondary metastatic tumours | Frequent | |||
| Lung carcinoma | 40c | Serous or fibrinous, frequently haemorrhagic effusion | ||
| Breast carcinoma | 22c | Accompanying disease during the infiltration of malignant cells | ||
| Gastric and colon | 3c | |||
| Other carcinoma | 6c | |||
| Leukemia and lymphoma | 15c | |||
| Melanoma | 3c | |||
| Sarcoma | 4c | |||
| Other tumours | 7c | |||
| Idiopathic | 3.5a, in other series \(>\) 50a | Serous, fibrinous, sometimes haemorrhagic PE with suspect viral or autoimmune secondary immunopathogenesis | ||
CHF, congestive heart failure; DDg, differential diagnosis; MI, myocardial infarction; P., pericarditis; PE, pericardial effusion.
Percentage related to the population of 260 subsequent patients undergoing pericardiocentesis, pericardioscopy and epicardial biopsy (Marburg pericarditis registry 1988–2001).1
Percentage related to the incidence of pericarditis in the specific population of patients (e.g., with systemic lupus erythematosus).
Percentage related to the population of patients with neoplastic pericarditis.
Pericardial syndromes
Congenital defects of the pericardium
Congenital defects of the pericardium (1/10.000 autopsies) comprise partial left (70%), right (17%) or total bilateral (rare) pericardial absence. Additional congenital abnormalities occur in ∼30% of patients.4 Most patients with a total pericardial absence are asymptomatic. Homolateral cardiac displacement and augmented heart mobility impose an increased risk for traumatic aortic dissection.5 Partial left side defects can be complicated by herniation and strangulation of the heart through the defect (chest pain, shortness of breath, syncope or sudden death). Surgical pericardioplasty (Dacron, Gore-tex, or bovine pericardium) is indicated for imminent strangulation.6
Acute pericarditis
Acute pericarditis is dry, fibrinous or effusive, independent from its aetiology. The diagnostic algorithm can be derived from Table 2.8–18 A prodrome of fever, malaise, and myalgia is common, but elderly patients may not be febrile. Major symptoms are retrosternal or left precordialchest pain (radiates to the trapezius ridge, can be pleuritic or simulate ischemia, and varies with posture) and shortness of breath. The pericardial friction rub can be transient, mono-, bi- or triphasic. Pleural effusion may be present. Heart rate is usually rapid and regular. Microvoltage and electrical alternans are reversible after effusion drainage.19 Echocardiography is essential to detect effusion, concomitant heart or paracardial disease.11,12
Diagnostic pathway and sequence of performance in acute pericarditis (level of evidence B for all procedures)
Technique | Characteristic findings | Reference | ||
|---|---|---|---|---|
| Obligatory (indication class I) | ||||
| Auscultation | Pericardial rub (mono-, bi-, or triphasic) | 7 | ||
| ECGa | Stage I: anterior and inferior concave ST segment elevation. PR segment deviations opposite to P polarity. | 7,19 | ||
| Early stage II: ST junctions return to the baseline, PR deviated. | ||||
| Late stage II: T waves progressively flatten and invert | ||||
| Stage III: generalised T wave inversions | ||||
| Stage IV: ECG returns to prepericarditis state. | ||||
| Echocardiography | Effusion types B–D (Horowitz) (Fig. 1) | 9,10 | ||
| Signs of tamponade (see Section Pericardial effusion and cardiac tamponde) | ||||
| Blood analyses | (a) ESR, CRP, LDH, leukocytes (inflammation markers) | 11 | ||
| (b) Troponin I, CK-MB (markers of myocardial lesion)b | ||||
| Chest X-ray | Ranging from normal to “water bottle” heart shadow. Revealing additional pulmonary/mediastinal pathology. | 12 | ||
| Mandatory in tamponade (indication class I), optional in large/recurrent effusions or if previous tests inconclusive (indication class IIa) in small: effusions (indication class IIb) | ||||
| Pericardiocentesis and drainage | PCR and histochemistry for aetiopathogenetic classification of infection or neoplasia | 2,8,13 | ||
| Optional or if previous tests inconclusive (indication class IIa) | ||||
| CT | Effusions, peri-, and epicardium | 14 | ||
| MRI | Effusions, peri-, and epicardium | 14 | ||
| Pericardioscopy, pericardial biopsy | Establishing the specific aetiology | 2,8,15,16 | ||
Technique | Characteristic findings | Reference | ||
|---|---|---|---|---|
| Obligatory (indication class I) | ||||
| Auscultation | Pericardial rub (mono-, bi-, or triphasic) | 7 | ||
| ECGa | Stage I: anterior and inferior concave ST segment elevation. PR segment deviations opposite to P polarity. | 7,19 | ||
| Early stage II: ST junctions return to the baseline, PR deviated. | ||||
| Late stage II: T waves progressively flatten and invert | ||||
| Stage III: generalised T wave inversions | ||||
| Stage IV: ECG returns to prepericarditis state. | ||||
| Echocardiography | Effusion types B–D (Horowitz) (Fig. 1) | 9,10 | ||
| Signs of tamponade (see Section Pericardial effusion and cardiac tamponde) | ||||
| Blood analyses | (a) ESR, CRP, LDH, leukocytes (inflammation markers) | 11 | ||
| (b) Troponin I, CK-MB (markers of myocardial lesion)b | ||||
| Chest X-ray | Ranging from normal to “water bottle” heart shadow. Revealing additional pulmonary/mediastinal pathology. | 12 | ||
| Mandatory in tamponade (indication class I), optional in large/recurrent effusions or if previous tests inconclusive (indication class IIa) in small: effusions (indication class IIb) | ||||
| Pericardiocentesis and drainage | PCR and histochemistry for aetiopathogenetic classification of infection or neoplasia | 2,8,13 | ||
| Optional or if previous tests inconclusive (indication class IIa) | ||||
| CT | Effusions, peri-, and epicardium | 14 | ||
| MRI | Effusions, peri-, and epicardium | 14 | ||
| Pericardioscopy, pericardial biopsy | Establishing the specific aetiology | 2,8,15,16 | ||
Typical lead involvement: I, II, aVL, aVF, and V3-V6. The ST segment is always depressed in aVR, frequently in V1, and occasionally in V2. Occasionally, stage IV does not occur and there are permanent T wave inversions and flattenings. If ECG is first recorded in stage III, pericarditis cannot be differentiated by ECG from diffuse myocardial injury, “biventricular strain,” or myocarditis. ECG in Early repolarization is very similar to stage I. Unlike stage I, this ECG does not acutely evolve and J-point elevations are usually accompanied by a slur, oscillation, or notch at the end of the QRS just before and including the J point (best seen with tall R and T waves – large in early repolarisation pattern). Pericarditis is likely if in lead V6 the J point is
Cardiac troponin I was detectable in 49% and
Diagnostic pathway and sequence of performance in acute pericarditis (level of evidence B for all procedures)
Technique | Characteristic findings | Reference | ||
|---|---|---|---|---|
| Obligatory (indication class I) | ||||
| Auscultation | Pericardial rub (mono-, bi-, or triphasic) | 7 | ||
| ECGa | Stage I: anterior and inferior concave ST segment elevation. PR segment deviations opposite to P polarity. | 7,19 | ||
| Early stage II: ST junctions return to the baseline, PR deviated. | ||||
| Late stage II: T waves progressively flatten and invert | ||||
| Stage III: generalised T wave inversions | ||||
| Stage IV: ECG returns to prepericarditis state. | ||||
| Echocardiography | Effusion types B–D (Horowitz) (Fig. 1) | 9,10 | ||
| Signs of tamponade (see Section Pericardial effusion and cardiac tamponde) | ||||
| Blood analyses | (a) ESR, CRP, LDH, leukocytes (inflammation markers) | 11 | ||
| (b) Troponin I, CK-MB (markers of myocardial lesion)b | ||||
| Chest X-ray | Ranging from normal to “water bottle” heart shadow. Revealing additional pulmonary/mediastinal pathology. | 12 | ||
| Mandatory in tamponade (indication class I), optional in large/recurrent effusions or if previous tests inconclusive (indication class IIa) in small: effusions (indication class IIb) | ||||
| Pericardiocentesis and drainage | PCR and histochemistry for aetiopathogenetic classification of infection or neoplasia | 2,8,13 | ||
| Optional or if previous tests inconclusive (indication class IIa) | ||||
| CT | Effusions, peri-, and epicardium | 14 | ||
| MRI | Effusions, peri-, and epicardium | 14 | ||
| Pericardioscopy, pericardial biopsy | Establishing the specific aetiology | 2,8,15,16 | ||
Technique | Characteristic findings | Reference | ||
|---|---|---|---|---|
| Obligatory (indication class I) | ||||
| Auscultation | Pericardial rub (mono-, bi-, or triphasic) | 7 | ||
| ECGa | Stage I: anterior and inferior concave ST segment elevation. PR segment deviations opposite to P polarity. | 7,19 | ||
| Early stage II: ST junctions return to the baseline, PR deviated. | ||||
| Late stage II: T waves progressively flatten and invert | ||||
| Stage III: generalised T wave inversions | ||||
| Stage IV: ECG returns to prepericarditis state. | ||||
| Echocardiography | Effusion types B–D (Horowitz) (Fig. 1) | 9,10 | ||
| Signs of tamponade (see Section Pericardial effusion and cardiac tamponde) | ||||
| Blood analyses | (a) ESR, CRP, LDH, leukocytes (inflammation markers) | 11 | ||
| (b) Troponin I, CK-MB (markers of myocardial lesion)b | ||||
| Chest X-ray | Ranging from normal to “water bottle” heart shadow. Revealing additional pulmonary/mediastinal pathology. | 12 | ||
| Mandatory in tamponade (indication class I), optional in large/recurrent effusions or if previous tests inconclusive (indication class IIa) in small: effusions (indication class IIb) | ||||
| Pericardiocentesis and drainage | PCR and histochemistry for aetiopathogenetic classification of infection or neoplasia | 2,8,13 | ||
| Optional or if previous tests inconclusive (indication class IIa) | ||||
| CT | Effusions, peri-, and epicardium | 14 | ||
| MRI | Effusions, peri-, and epicardium | 14 | ||
| Pericardioscopy, pericardial biopsy | Establishing the specific aetiology | 2,8,15,16 | ||
Typical lead involvement: I, II, aVL, aVF, and V3-V6. The ST segment is always depressed in aVR, frequently in V1, and occasionally in V2. Occasionally, stage IV does not occur and there are permanent T wave inversions and flattenings. If ECG is first recorded in stage III, pericarditis cannot be differentiated by ECG from diffuse myocardial injury, “biventricular strain,” or myocarditis. ECG in Early repolarization is very similar to stage I. Unlike stage I, this ECG does not acutely evolve and J-point elevations are usually accompanied by a slur, oscillation, or notch at the end of the QRS just before and including the J point (best seen with tall R and T waves – large in early repolarisation pattern). Pericarditis is likely if in lead V6 the J point is
Cardiac troponin I was detectable in 49% and
Perimyocarditis is evidenced by global or regional myocardial dysfunction, elevations of troponins I and T, MB creatine-kinase, myoglobin and tumour necrosis factor. Auscultation of a new S3 heart sound, convexly elevated J-ST segment in the ECG, fixation of Indium-111-labelled antimyosin antibodies, and structural changes in MRI are indicative, but only endomyocardial/epimyocardial biopsy is diagnostic.7,8
Hospitalisation is warranted to determine the aetiology and observe for tamponade as well as the effect of treatment. Nonsteroidal anti-inflammatory drugs (NSAID) are the mainstay (level of evidence B, class I). Indomethacine should be avoided in elderly patients due to its flow reduction in the coronaries. Ibuprofen is preferred for its rare side-effects, favourable impact on the coronary flow, and the large dose range.7 Depending on severity and response, 300–800 mg every 6–8 hours may be initially required and can be continued for days or weeks, best until the effusion has disappeared. Gastrointestinal protection must be provided. Colchicine (0.5 mg bid) added to an NSAID or as monotherapy also appears to be effective for the initial attack and the prevention of recurrences (level of evidence B, class IIa indication).20 It is well tolerated with fewer side effects than NSAIDs. Systemic corticosteroid therapy should be restricted to connective tissue diseases, autoreactive or uremic pericarditis. Intrapericardial application avoids systemic side effects and is highly effective (level of evidence B, class IIa indication).2 For tapering of prednisone, ibuprofen or colchicine should be introduced early.20 Indications for pericardiocentesis are listed in Focus box 1.7,21–30 Recovered patients should be observed for recurrences or constriction.
Chronic pericarditis
Chronic (
Recurrent pericarditis
The term recurrent pericarditis encompasses (1) the intermittent type (symptom free intervals without therapy) and (2) the incessant type (discontinuation of anti-inflammatory therapy ensures a relapse). Massive pericardial effusion, overt tamponade or constriction are rare. Evidence for an immunopathological process include: (1) the latent period lasting for months; (2) the presence of anti-heart antibodies; (3) the quick response to steroid treatment and the similarity and co-existence of recurrent pericarditis with other autoimmune conditions (lupus, serum sickness, polyserositis, postpericardiotomy/postmyocardial infarction syndrome, celiac disease, dermatitis herpetiformis, frequent arthralgias, eosinophilia, allergic drug reaction, and history of allergy). Potential underlying genetic disorders were also reported: autosomal dominant inheritance with incomplete penetrance32 and sex-linked inheritance (recurrent pericarditis associated with ocular hypertension).33
Symptomatic management relies on exercise restriction and the regimen used in acute pericarditis. Colchicine was effective when NSAIDs and corticosteroids failed to prevent relapses.20,34–35 During 1004 months of colchicine treatment, only 13.7% new recurrences occurred.20 During the 2333 months of follow-up, 60.7% of the patients remained recurrence-free. The recommended dose is 2 mg/day for one or two days, followed by 1 mg/day (level of evidence B, indication I). Corticosteroids should be used only in patients with poor general condition or in frequent crises7 (level of evidence C, indication IIa). A common mistake is to use a dose too low to be effective or to taper the dose too rapidly. The recommended regimen is: prednisone 1–1.5 mg/kg, for at least one month. If patients do not respond adequately, azathioprine (75–100 mg/day) or cyclophosphamide can be added.36 Corticoids should be tapered over a three-month period. If symptoms still recur, return to the last dose that suppressed the manifestations, maintain that dose for 2–3 weeks and then recommence tapering. Towards the end of the taper, introduce anti-inflammatory treatment with colchicine or NSAID. Renewed treatment should continue for at least three months. Pericardiectomy is indicated only in frequent and highly symptomatic recurrences resistant to medical treatment (level of evidence B, indication IIa).37 Before pericardiectomy, the patient should be on a steroid-free regimen for several weeks. Post pericardiectomy recurrences were also demonstrated, possibly due to incomplete resection of the pericardium.
Pericardial effusion and cardiac tamponade
Pericardial effusion may appear as transudate (hydropericardium), exudate, pyopericardium or haemopericardium. Large effusions are common with neoplastic, tuberculous, cholesterol, uremic pericarditis, myxedema, and parasitoses.38 Effusions that develop slowly can be remarkably asymptomatic, while rapidly accumulating smaller effusions can present with tamponade. Loculated effusions are more common when scarring has supervened (e.g., postsurgical, posttrauma, purulent pericarditis). Massive chronic pericardial effusions are rare (2–3.5% of all large effusions).39Cardiac tamponade is the decompensated phase of cardiac compression caused by effusion accumulation and the increased intrapericardial pressure. In “surgical” tamponade intrapericardial pressure is rising rapidly, in the matter of minutes to hours (i.e. haemorrhage), whereas a low-intensity inflammatory process is developing days to weeks before cardiac compression occurs (“medical” tamponade). Heart sounds are distant. Orthopnoea, cough and dysphagia, occasionally with episodes of unconsciousness can be observed. Insidiously developing tamponade may present with the signs of its complications (renal failure, abdominal plethora, shock liver and mesenteric ischemia). In 60% of the patients, the cause of pericardial effusion may be a known medical condition.40 Tamponade without two or more inflammatory signs (typical pain, pericardial friction rub, fever, diffuse ST segment elevation) is usually associated with a malignant effusion (likelihood ratio 2.9). Electrocardiography may demonstrate diminished QRS and T-wave voltages, PR-segment depression, ST-T changes, bundle branch block, and electrical alternans (rarely seen in the absence of tamponade).7 In chest radiography large effusions are depicted as globular cardiomegaly with sharp margins (“water bottle” silhouette).12 On well-penetrated lateral radiographies, or cine films, pericardial fluid is suggested by lucent lines within the cardiopericardial shadow (epicardial halo).12,41,42 This sign is useful for the fluoroscopic guidance of pericardiocentesis.27 The separation of pericardial layers can be detected in echocardiography, when the pericardial fluid exceeds 15–35 ml (Fig. 1).43 The size of effusions can be graded as: (1) small (echo-free space in diastole
![Horowitz classification of pericardial effusions.43 Type A: No effusion; Type B: Separation of epicardium and pericardium (3–16 ml); Type C 1: Systolic and diastolic separation of epicardium and pericardium (small effusion \batchmode \documentclass[fleqn,10pt,legalpaper]{article} \usepackage{amssymb} \usepackage{amsfonts} \usepackage{amsmath} \pagestyle{empty} \begin{document} \(>\) \end{document}16 ml); Type C 2: Systolic and diastolic separation of epicardium and pericardium with attenuated pericardial motion; Type D: Pronounced separation of epicardium and pericardium with large echo-free space; Type E: Pericardial thickening (\batchmode \documentclass[fleqn,10pt,legalpaper]{article} \usepackage{amssymb} \usepackage{amsfonts} \usepackage{amsmath} \pagestyle{empty} \begin{document} \(>\) \end{document}4 mm). Copyrights American Heart Association.](https://oup.silverchair-cdn.com/oup/backfile/Content_public/Journal/eurheartj/25/7/10.1016_j.ehj.2004.02.002/2/m_4000673.587.GR1.jpeg?Expires=1716313867&Signature=oY~wE2E2TyRdB32L5ndLqkoPjabjg2~C~Mz2egC4T-nZffcRnnvaIZ~ClQH~Xcw0RaNdN5gW5s7brTWsZC4QALVSlMQF7gxoHHAZrCJ9T2NcFhkt09eHEEaPRWU2FtZDTnNCIXNS-BEwHx7NlI-bZZs8k5r04MYqnrTNoRjuRsZmm9QThAyKDubdMzNJFKrbQfKvOUeKqT-38YM7rmez315w30agfYCIlB7nAxlxrJ8x4Hq2E8sW1JxbX-eJpcFR-JukuSJqvVyFryEdjJmXflo8V~jDE0n7zJErwps0k-t-5yNqUuN1ZM~oYlTMOxbYiiPI9Vj0P2613GGWVGINSA__&Key-Pair-Id=APKAIE5G5CRDK6RD3PGA)
Horowitz classification of pericardial effusions.43 Type A: No effusion; Type B: Separation of epicardium and pericardium (3–16 ml); Type C 1: Systolic and diastolic separation of epicardium and pericardium (small effusion
Diagnosis of cardiac tamponade
Clinical presentation | Elevated systemic venous pressurea, hypotensionb, pulsus paradoxusc, tachycardiad, dyspnoea or tachypnoea with clear lungs |
| Precipitating factors | Drugs (cyclosporine, anticoagulants, thrombolytics, etc.), recent cardiac surgery, indwelling instrumentation, blunt chest trauma, malignancies, connective tissue disease, renal failure, septicaemiae |
| ECG | Can be normal or non-specifically changed (ST-T wave), electrical alternans (QRS, rarely T), bradycardi (end-stage), Electromechanical dissociation (agonal phase) |
| Chest X-ray | Enlarged cardiac silhouette with clear lungs. |
| M mode/2D echocardiogram | Diastolic collapse of the (1) anterior RV free wall52f, RA collapse53, LA54 and very rarely LV55 collapse, increased LV diastolic wall thickness “pseudohypertrophy”56, VCI dilatation (no collapse in inspirium), “swinging heart”57 |
| Doppler | Tricuspid flow increases and mitral flow decreases during inspiration (reverse in expiration) |
| Systolic and diastolic flows are reduced in systemic veins in expirium and reverse flow with atrial contraction is increased58 | |
| M-mode colour Doppler | Large respiratory fluctuations in mitral/tricuspid flows59 |
| Cardiac catheterisation | (1) Confirmation of the diagnosis and quantification of the haemodynamic compromise60 |
| RA pressure is elevated (preserved systolic x descent and absent or diminished diastolic y descent) | |
| Intrapericardial pressure is also elevated and virtually identical to RA pressure (both pressures fall in inspiration) | |
| RV mid-diastolic pressure elevated and equal to the RA and pericardial pressures (no dip-and-plateau configuration) | |
| Pulmonary artery diastolic pressure is slightly elevated and may correspond to the RV pressure. | |
| Pulmonary capillary wedge pressure is also elevated and nearly equal to intrapericardial and right atrial pressure. | |
| LV systolic and aortic pressures may be normal or reduced. | |
| (2) Documenting that pericardial aspiration is followed by haemodynamic improvementg | |
| (3) Detection of the coexisting haemodynamic abnormalities (LV failure, constriction, pulmonary hypertension) | |
| (4) Detection of associated cardiovascular diseases (cardiomyopathy, coronary artery disease) | |
| RV/LV angiography | Atrial collapse and small hyperactive ventricular chambers. |
| Coronary angiography | Coronary compression in diastole. |
| Computer tomography | No visualisation of subepicardial fat along both ventricles, which show tube-like configuration and anteriorly drawn atrias |
Clinical presentation | Elevated systemic venous pressurea, hypotensionb, pulsus paradoxusc, tachycardiad, dyspnoea or tachypnoea with clear lungs |
| Precipitating factors | Drugs (cyclosporine, anticoagulants, thrombolytics, etc.), recent cardiac surgery, indwelling instrumentation, blunt chest trauma, malignancies, connective tissue disease, renal failure, septicaemiae |
| ECG | Can be normal or non-specifically changed (ST-T wave), electrical alternans (QRS, rarely T), bradycardi (end-stage), Electromechanical dissociation (agonal phase) |
| Chest X-ray | Enlarged cardiac silhouette with clear lungs. |
| M mode/2D echocardiogram | Diastolic collapse of the (1) anterior RV free wall52f, RA collapse53, LA54 and very rarely LV55 collapse, increased LV diastolic wall thickness “pseudohypertrophy”56, VCI dilatation (no collapse in inspirium), “swinging heart”57 |
| Doppler | Tricuspid flow increases and mitral flow decreases during inspiration (reverse in expiration) |
| Systolic and diastolic flows are reduced in systemic veins in expirium and reverse flow with atrial contraction is increased58 | |
| M-mode colour Doppler | Large respiratory fluctuations in mitral/tricuspid flows59 |
| Cardiac catheterisation | (1) Confirmation of the diagnosis and quantification of the haemodynamic compromise60 |
| RA pressure is elevated (preserved systolic x descent and absent or diminished diastolic y descent) | |
| Intrapericardial pressure is also elevated and virtually identical to RA pressure (both pressures fall in inspiration) | |
| RV mid-diastolic pressure elevated and equal to the RA and pericardial pressures (no dip-and-plateau configuration) | |
| Pulmonary artery diastolic pressure is slightly elevated and may correspond to the RV pressure. | |
| Pulmonary capillary wedge pressure is also elevated and nearly equal to intrapericardial and right atrial pressure. | |
| LV systolic and aortic pressures may be normal or reduced. | |
| (2) Documenting that pericardial aspiration is followed by haemodynamic improvementg | |
| (3) Detection of the coexisting haemodynamic abnormalities (LV failure, constriction, pulmonary hypertension) | |
| (4) Detection of associated cardiovascular diseases (cardiomyopathy, coronary artery disease) | |
| RV/LV angiography | Atrial collapse and small hyperactive ventricular chambers. |
| Coronary angiography | Coronary compression in diastole. |
| Computer tomography | No visualisation of subepicardial fat along both ventricles, which show tube-like configuration and anteriorly drawn atrias |
LA, left atrium, LV, left ventricle, RA, right atrium, RV, right ventricle, VCI, inferior vena cava.
Jugular venous distension is less notable in hypovolemic patients or in “surgical tamponade”. An inspiratory increase or lack of fall of the pressure in the neck veins (Kussmaul sign), when verified with tamponade, or after pericardial drainage, indicates effusive-constrictive disease.
Heart rate is usually >100 beats/min, but may be lower in hypothyroidism and in uremic patients.
Pulsus paradoxus is absent in tamponade complicating atrial septal defect61 and in patients with significant aortic regurgitation.
Occasional patients are hypertensive especially if they have pre-existing hypertension.62
Febrile tamponade may be misdiagnosed as septic shock.
Right ventricular collapse can be absent in elevated right ventricular pressure and right ventricular hypertrophy63 or in right ventricular infarction.
If after drainage of pericardial effusion intrapericardial pressure does not fall below atrial pressure, the effusive-constrictive disease should be considered.
Diagnosis of cardiac tamponade
Clinical presentation | Elevated systemic venous pressurea, hypotensionb, pulsus paradoxusc, tachycardiad, dyspnoea or tachypnoea with clear lungs |
| Precipitating factors | Drugs (cyclosporine, anticoagulants, thrombolytics, etc.), recent cardiac surgery, indwelling instrumentation, blunt chest trauma, malignancies, connective tissue disease, renal failure, septicaemiae |
| ECG | Can be normal or non-specifically changed (ST-T wave), electrical alternans (QRS, rarely T), bradycardi (end-stage), Electromechanical dissociation (agonal phase) |
| Chest X-ray | Enlarged cardiac silhouette with clear lungs. |
| M mode/2D echocardiogram | Diastolic collapse of the (1) anterior RV free wall52f, RA collapse53, LA54 and very rarely LV55 collapse, increased LV diastolic wall thickness “pseudohypertrophy”56, VCI dilatation (no collapse in inspirium), “swinging heart”57 |
| Doppler | Tricuspid flow increases and mitral flow decreases during inspiration (reverse in expiration) |
| Systolic and diastolic flows are reduced in systemic veins in expirium and reverse flow with atrial contraction is increased58 | |
| M-mode colour Doppler | Large respiratory fluctuations in mitral/tricuspid flows59 |
| Cardiac catheterisation | (1) Confirmation of the diagnosis and quantification of the haemodynamic compromise60 |
| RA pressure is elevated (preserved systolic x descent and absent or diminished diastolic y descent) | |
| Intrapericardial pressure is also elevated and virtually identical to RA pressure (both pressures fall in inspiration) | |
| RV mid-diastolic pressure elevated and equal to the RA and pericardial pressures (no dip-and-plateau configuration) | |
| Pulmonary artery diastolic pressure is slightly elevated and may correspond to the RV pressure. | |
| Pulmonary capillary wedge pressure is also elevated and nearly equal to intrapericardial and right atrial pressure. | |
| LV systolic and aortic pressures may be normal or reduced. | |
| (2) Documenting that pericardial aspiration is followed by haemodynamic improvementg | |
| (3) Detection of the coexisting haemodynamic abnormalities (LV failure, constriction, pulmonary hypertension) | |
| (4) Detection of associated cardiovascular diseases (cardiomyopathy, coronary artery disease) | |
| RV/LV angiography | Atrial collapse and small hyperactive ventricular chambers. |
| Coronary angiography | Coronary compression in diastole. |
| Computer tomography | No visualisation of subepicardial fat along both ventricles, which show tube-like configuration and anteriorly drawn atrias |
Clinical presentation | Elevated systemic venous pressurea, hypotensionb, pulsus paradoxusc, tachycardiad, dyspnoea or tachypnoea with clear lungs |
| Precipitating factors | Drugs (cyclosporine, anticoagulants, thrombolytics, etc.), recent cardiac surgery, indwelling instrumentation, blunt chest trauma, malignancies, connective tissue disease, renal failure, septicaemiae |
| ECG | Can be normal or non-specifically changed (ST-T wave), electrical alternans (QRS, rarely T), bradycardi (end-stage), Electromechanical dissociation (agonal phase) |
| Chest X-ray | Enlarged cardiac silhouette with clear lungs. |
| M mode/2D echocardiogram | Diastolic collapse of the (1) anterior RV free wall52f, RA collapse53, LA54 and very rarely LV55 collapse, increased LV diastolic wall thickness “pseudohypertrophy”56, VCI dilatation (no collapse in inspirium), “swinging heart”57 |
| Doppler | Tricuspid flow increases and mitral flow decreases during inspiration (reverse in expiration) |
| Systolic and diastolic flows are reduced in systemic veins in expirium and reverse flow with atrial contraction is increased58 | |
| M-mode colour Doppler | Large respiratory fluctuations in mitral/tricuspid flows59 |
| Cardiac catheterisation | (1) Confirmation of the diagnosis and quantification of the haemodynamic compromise60 |
| RA pressure is elevated (preserved systolic x descent and absent or diminished diastolic y descent) | |
| Intrapericardial pressure is also elevated and virtually identical to RA pressure (both pressures fall in inspiration) | |
| RV mid-diastolic pressure elevated and equal to the RA and pericardial pressures (no dip-and-plateau configuration) | |
| Pulmonary artery diastolic pressure is slightly elevated and may correspond to the RV pressure. | |
| Pulmonary capillary wedge pressure is also elevated and nearly equal to intrapericardial and right atrial pressure. | |
| LV systolic and aortic pressures may be normal or reduced. | |
| (2) Documenting that pericardial aspiration is followed by haemodynamic improvementg | |
| (3) Detection of the coexisting haemodynamic abnormalities (LV failure, constriction, pulmonary hypertension) | |
| (4) Detection of associated cardiovascular diseases (cardiomyopathy, coronary artery disease) | |
| RV/LV angiography | Atrial collapse and small hyperactive ventricular chambers. |
| Coronary angiography | Coronary compression in diastole. |
| Computer tomography | No visualisation of subepicardial fat along both ventricles, which show tube-like configuration and anteriorly drawn atrias |
LA, left atrium, LV, left ventricle, RA, right atrium, RV, right ventricle, VCI, inferior vena cava.
Jugular venous distension is less notable in hypovolemic patients or in “surgical tamponade”. An inspiratory increase or lack of fall of the pressure in the neck veins (Kussmaul sign), when verified with tamponade, or after pericardial drainage, indicates effusive-constrictive disease.
Heart rate is usually >100 beats/min, but may be lower in hypothyroidism and in uremic patients.
Pulsus paradoxus is absent in tamponade complicating atrial septal defect61 and in patients with significant aortic regurgitation.
Occasional patients are hypertensive especially if they have pre-existing hypertension.62
Febrile tamponade may be misdiagnosed as septic shock.
Right ventricular collapse can be absent in elevated right ventricular pressure and right ventricular hypertrophy63 or in right ventricular infarction.
If after drainage of pericardial effusion intrapericardial pressure does not fall below atrial pressure, the effusive-constrictive disease should be considered.
Pericardiocentesis is not necessary when the diagnosis can be made otherwise or the effusions are small or resolving under anti-inflammatory treatment. Haemodynamic compromise and cardiac tamponade is an absolute indication for drainage (Focus box 1). Patients with dehydration and hypovolemia may temporarily improve with intravenous fluids. Whenever possible, treatment should be aimed at the underlying aetiology. Even in idiopathic effusions extended pericardial catheter drainage (3±2 days, range 1–13 days) was associated with a lower recurrence rates (6% vs. 23%) than in those without catheter drainage during the follow-up of 3.8±4.3 years.25 Resistant neoplastic processes require intrapericardial treatment,63 percutaneous balloon pericardiotomy31 or rarely pericardiectomy. Surgical approach is recommended only in patients with very large chronic effusion in whom repeated pericardiocentesis and/or intrapericardial therapy were not successful.64
Constrictive pericarditis
Constrictive pericarditis is a rare but severely disabling consequence of the chronic inflammation of the pericardium, leading to an impaired filling of the ventricles and reduced ventricular function. Until recently, increased pericardial thickness has been considered an essential diagnostic feature of constrictive pericarditis. However, in the large surgical series from the Mayo clinic constriction was present in 18% of the patients with normal pericardial thickness.65 Tuberculosis, mediastinal irradiation, and previous cardiac surgical procedures are frequent causes of the disease, which can present in several pathoanatomical forms66 (Fig. 2). Constrictive pericarditis may rarely develop only in the epicardial layer in patients with previously removed parietal pericardium.67 Transient constrictive pericarditis is uncommon but important entity, since these patients are not indicated for pericardiectomy.68 Patients complain about fatigue, peripheral oedema, breathlessness, and abdominal swelling, which may be aggravated by a protein-loosing enteropathy. Typically, there is a long delay between the initial pericardial inflammation and the onset of constriction. In decompensated patients venous congestion, hepatomegaly, pleural effusions, and ascites may occur. Haemodynamic impairment of the patient can be additionally aggravated by a systolic dysfunction due to myocardial fibrosis or atrophy. Clinical, echocardiographic, and haemodynamic parameters can be derived from Table 4.50,65,66,69–71 Differential diagnosis has to include acute dilatation of the heart, pulmonary embolism, right ventricular infarction, pleural effusion, chronic obstructive lung diseases72 and restrictive cardiomyopathy. The best way to distinguish constrictive pericarditis from restrictive cardiomyopathy is the analysis of respiratory changes with or without changes of preload by Doppler and/or tissue Doppler echocardiography,73 but physical findings, ECG, chest radiography, CT and MRI, haemodynamics, and endomyocardial biopsy may be helpful as well.7
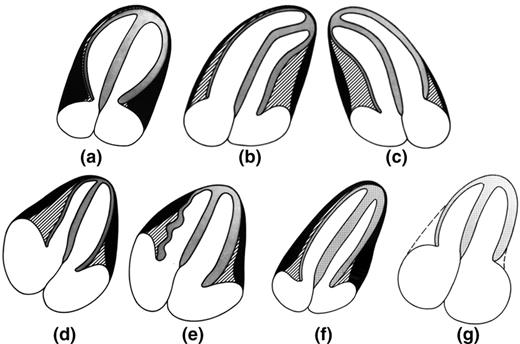
Pathoanatomical forms of constrictive pericarditis vs. restrictive cardiomyopathy. (a) Annular form of pericardial constriction with bilateral thickening of the pericardium along the atrial ventricular grooves with normal configuration of both ventricles and enlargement of both atria. (b) Left sided form of pericardial constriction with thickened pericardium along the left ventricle and right sided bending of the interventricular septum with tube-like configuration of mainly left ventricle and enlargement of both atria. (lateral sternotomy and partial pericardiectomy is indicated). (c) Right sided form of pericardial constriction with thickened pericardium along the right ventricle and left sided bending of the interventricular septum with tube-like configuration of mainly right ventricle and enlargement of both atria (median sternotomy and partial pericardiectomy is indicated). (d) Myocardial atrophy and global form of pericardial constriction with bilateral thickening of the pericardium along both ventricles separated from the right myocardial wall by a thin layer of subepicardial fat. Tube-like configuration of both ventricles and enlargement of both atria, however, thinning of the interventricular septum and posterolateral wall of the left ventricle below 1 cm is suggesting myocardial atrophy (pericardiectomy is contraindicated). (e) Perimyocardial fibrosis and global form of pericardial constriction with bilateral thickening of the pericardium along both ventricles, however, the right sided thickened pericardium cannot be separated from the wave-like thin form of right sided ventricular wall suggesting perimyocardial fibrosis (pericardiectomy is contraindicated). (f) Global form of pericardial constriction with bilateral thickening of the pericardium along both ventricles separated from the right myocardial wall by a thin layer of subepicardial fat. Tube-like configuration of both ventricles and enlargement of both atria (median sternotomy and pericardiectomy is indicated). (g) Restrictive cardiomyopathy with normal thin pericardium along both ventricles that show normal configuration and with enlargement of both atria.
Diagnostic approach in constrictive pericarditis
Clinical presentation | Severe chronic systemic venous congestion associated with low cardiac output, including jugular venous distension, hypotension with a low pulse pressure, abdominal distension, oedema and muscle wasting |
| ECG | Can be normal, or reveal low QRS voltage, generalized T-wave inversion/flattening, LA abnormalities, atrial fibrillation, atrioventricular block, intraventricular conduction defects, or rarely pseudoinfarction pattern |
| Chest X-ray | Pericardial calcifications, pleural effusions |
| M mode/2D echocardiogram | Pericardial thickening and calcificationsa as well as the indirect signs of constriction: |
| RA&LA enlargement with normal appearance of the ventricles, and normal systolic function | |
| Early pathological outward and inward movement of the interventricular septum (“dip-plateau phenomenon”)72 | |
| Flattering waves at the LV posterior wall | |
| LV diameter is not increasing after the early rapid filling phase | |
| VCI and the hepatic veins are dilated with restricted respiratory fluctuationsb | |
| Doppler | Restricted filling of both ventricles with respiratory variation \(>\) 25% over the AV-valves)69c |
| TEE | Measurement of the pericardial thickness50 |
| CT/MRI | Thickened and/or calcified pericardium, tube-like configuration of one or both ventricles, narrowing of one or both atrio-ventricular grooves, congestion of the caval veins66 enlargement of one or both atria |
| Cardiac catheterisation | “Dip and plateau” or “square route” sign in the pressure curve of the right and/or left ventricle |
| Equalisation of LV/RV end-diastolic pressures in the range of 5 mmHg or less72d | |
| RV/LV angiography | The reduction of RV&LV size and increase of RA&LA size |
| During diastole a rapid early filling with stop of further enlargement (“dip-plateau”) | |
| Coronary angiography | In all patients over 35 years and in patients with a history of mediastinal irradiation, regardless of the age |
Clinical presentation | Severe chronic systemic venous congestion associated with low cardiac output, including jugular venous distension, hypotension with a low pulse pressure, abdominal distension, oedema and muscle wasting |
| ECG | Can be normal, or reveal low QRS voltage, generalized T-wave inversion/flattening, LA abnormalities, atrial fibrillation, atrioventricular block, intraventricular conduction defects, or rarely pseudoinfarction pattern |
| Chest X-ray | Pericardial calcifications, pleural effusions |
| M mode/2D echocardiogram | Pericardial thickening and calcificationsa as well as the indirect signs of constriction: |
| RA&LA enlargement with normal appearance of the ventricles, and normal systolic function | |
| Early pathological outward and inward movement of the interventricular septum (“dip-plateau phenomenon”)72 | |
| Flattering waves at the LV posterior wall | |
| LV diameter is not increasing after the early rapid filling phase | |
| VCI and the hepatic veins are dilated with restricted respiratory fluctuationsb | |
| Doppler | Restricted filling of both ventricles with respiratory variation \(>\) 25% over the AV-valves)69c |
| TEE | Measurement of the pericardial thickness50 |
| CT/MRI | Thickened and/or calcified pericardium, tube-like configuration of one or both ventricles, narrowing of one or both atrio-ventricular grooves, congestion of the caval veins66 enlargement of one or both atria |
| Cardiac catheterisation | “Dip and plateau” or “square route” sign in the pressure curve of the right and/or left ventricle |
| Equalisation of LV/RV end-diastolic pressures in the range of 5 mmHg or less72d | |
| RV/LV angiography | The reduction of RV&LV size and increase of RA&LA size |
| During diastole a rapid early filling with stop of further enlargement (“dip-plateau”) | |
| Coronary angiography | In all patients over 35 years and in patients with a history of mediastinal irradiation, regardless of the age |
LA, left atrium, LV, left ventricle, RA, right atrium, RV, right ventricle, VCI, inferior vena cava, TEE – transoesophageal echocardiography
e In chronic obstructive lung disease mitral in-flow velocity will decrease nearly 100% during inspiration and increase during expiration. The mitral E-velocity is highest at the end of expiration (in constrictive pericarditis mitral E-velocity is highest immediately after start of expiration).71 In addition, superior vena cava flow increases with inspiration in chronic obstructive lung disease, whereas it does not change significantly with respiration in constrictive pericarditis.
Thickening of the pericardium is not always equal to constriction (absent in 18% of 143 surgically proven cases). When clinical, echocardiographic, or invasive haemodynamic features indicate constriction, pericardiectomy should not be denied on the basis of normal pericardial thickness.65
Diagnosis is difficult in atrial fibrillation. Hepatic diastolic vein flow reversal in expirium is observed even when the flow velocity pattern is inconclusive.69
Patients with increased atrial pressures or mixed constriction and restriction demonstrate <25% respiratory changes.72 A provocation test with head-up tilting or sitting position with decrease of preload may unmask the constrictive pericarditis.70
In the early stage or in the occult form, these signs may not be present and the rapid infusion of 1–2 l of normal saline may be necessary to establish the diagnosis. Constrictive haemodynamics may be masked or complicated by valvular- and coronary artery disease.
Diagnostic approach in constrictive pericarditis
Clinical presentation | Severe chronic systemic venous congestion associated with low cardiac output, including jugular venous distension, hypotension with a low pulse pressure, abdominal distension, oedema and muscle wasting |
| ECG | Can be normal, or reveal low QRS voltage, generalized T-wave inversion/flattening, LA abnormalities, atrial fibrillation, atrioventricular block, intraventricular conduction defects, or rarely pseudoinfarction pattern |
| Chest X-ray | Pericardial calcifications, pleural effusions |
| M mode/2D echocardiogram | Pericardial thickening and calcificationsa as well as the indirect signs of constriction: |
| RA&LA enlargement with normal appearance of the ventricles, and normal systolic function | |
| Early pathological outward and inward movement of the interventricular septum (“dip-plateau phenomenon”)72 | |
| Flattering waves at the LV posterior wall | |
| LV diameter is not increasing after the early rapid filling phase | |
| VCI and the hepatic veins are dilated with restricted respiratory fluctuationsb | |
| Doppler | Restricted filling of both ventricles with respiratory variation \(>\) 25% over the AV-valves)69c |
| TEE | Measurement of the pericardial thickness50 |
| CT/MRI | Thickened and/or calcified pericardium, tube-like configuration of one or both ventricles, narrowing of one or both atrio-ventricular grooves, congestion of the caval veins66 enlargement of one or both atria |
| Cardiac catheterisation | “Dip and plateau” or “square route” sign in the pressure curve of the right and/or left ventricle |
| Equalisation of LV/RV end-diastolic pressures in the range of 5 mmHg or less72d | |
| RV/LV angiography | The reduction of RV&LV size and increase of RA&LA size |
| During diastole a rapid early filling with stop of further enlargement (“dip-plateau”) | |
| Coronary angiography | In all patients over 35 years and in patients with a history of mediastinal irradiation, regardless of the age |
Clinical presentation | Severe chronic systemic venous congestion associated with low cardiac output, including jugular venous distension, hypotension with a low pulse pressure, abdominal distension, oedema and muscle wasting |
| ECG | Can be normal, or reveal low QRS voltage, generalized T-wave inversion/flattening, LA abnormalities, atrial fibrillation, atrioventricular block, intraventricular conduction defects, or rarely pseudoinfarction pattern |
| Chest X-ray | Pericardial calcifications, pleural effusions |
| M mode/2D echocardiogram | Pericardial thickening and calcificationsa as well as the indirect signs of constriction: |
| RA&LA enlargement with normal appearance of the ventricles, and normal systolic function | |
| Early pathological outward and inward movement of the interventricular septum (“dip-plateau phenomenon”)72 | |
| Flattering waves at the LV posterior wall | |
| LV diameter is not increasing after the early rapid filling phase | |
| VCI and the hepatic veins are dilated with restricted respiratory fluctuationsb | |
| Doppler | Restricted filling of both ventricles with respiratory variation \(>\) 25% over the AV-valves)69c |
| TEE | Measurement of the pericardial thickness50 |
| CT/MRI | Thickened and/or calcified pericardium, tube-like configuration of one or both ventricles, narrowing of one or both atrio-ventricular grooves, congestion of the caval veins66 enlargement of one or both atria |
| Cardiac catheterisation | “Dip and plateau” or “square route” sign in the pressure curve of the right and/or left ventricle |
| Equalisation of LV/RV end-diastolic pressures in the range of 5 mmHg or less72d | |
| RV/LV angiography | The reduction of RV&LV size and increase of RA&LA size |
| During diastole a rapid early filling with stop of further enlargement (“dip-plateau”) | |
| Coronary angiography | In all patients over 35 years and in patients with a history of mediastinal irradiation, regardless of the age |
LA, left atrium, LV, left ventricle, RA, right atrium, RV, right ventricle, VCI, inferior vena cava, TEE – transoesophageal echocardiography
e In chronic obstructive lung disease mitral in-flow velocity will decrease nearly 100% during inspiration and increase during expiration. The mitral E-velocity is highest at the end of expiration (in constrictive pericarditis mitral E-velocity is highest immediately after start of expiration).71 In addition, superior vena cava flow increases with inspiration in chronic obstructive lung disease, whereas it does not change significantly with respiration in constrictive pericarditis.
Thickening of the pericardium is not always equal to constriction (absent in 18% of 143 surgically proven cases). When clinical, echocardiographic, or invasive haemodynamic features indicate constriction, pericardiectomy should not be denied on the basis of normal pericardial thickness.65
Diagnosis is difficult in atrial fibrillation. Hepatic diastolic vein flow reversal in expirium is observed even when the flow velocity pattern is inconclusive.69
Patients with increased atrial pressures or mixed constriction and restriction demonstrate <25% respiratory changes.72 A provocation test with head-up tilting or sitting position with decrease of preload may unmask the constrictive pericarditis.70
In the early stage or in the occult form, these signs may not be present and the rapid infusion of 1–2 l of normal saline may be necessary to establish the diagnosis. Constrictive haemodynamics may be masked or complicated by valvular- and coronary artery disease.
Pericardiectomy is the only treatment for permanent constriction. The indications are based upon clinical symptoms, echocardiography findings, CT/MRI, and heart catheterisation. There are two standard approaches, both aiming at resecting the diseased pericardium as far as possible:74–77 (1) The antero-lateral thoracotomy (fifth intercostal space) and (2) median sternotomy (faster access to the aorta and right atrium for extracorporeal circulation). A primary installation of cardiopulmonary bypass is not recommended (diffuse bleeding following systemic heparinisation). If severe calcified adhesions between peri- and epicardium or a general affection of the epicardium (“outer porcelain heart”) are present surgery carries a high risk of either incomplete success or severe myocardial damage. An alternative approach in such cases may be a “laser shaving” using an Excimer laser.75 Areas of strong calcification or dense scaring may be left as islands to avoid major bleeding. Pericardiectomy for constrictive pericarditis has a mortality rate of 6–12%.75,77 The complete normalization of cardiac haemodynamics is reported in only 60% of the patients.74,76 The deceleration time (DT) may remain prolonged78 and postoperative respiratory variations of mitral/tricuspid flow are found in 9–25%.76,79 Left ventricular ejection fraction can increase due to a better ventricular filling.76,78 Major complications include acute perioperative cardiac insufficiency and ventricular wall rupture.80 Cardiac mortality and morbidity at pericardiectomy is mainly caused by the pre-surgically unrecognised presence of myocardial atrophy or myocardial fibrosis (Fig. 2).66 Exclusion of patients with extensive myocardial fibrosis and/or atrophy reduced the mortality rate for pericardiectomy to 5%. Postoperative low cardiac output80 should be treated by fluid substitution and catecholamines, high doses of digitalis, and intraaortic balloon pump in most severe cases. If indication for surgery was established early, long-term survival after pericardiectomy corresponds to that of the general population.75,76 However, if severe clinical symptoms were present for a longer period before surgery, even a complete pericardiectomy may not achieve a total restitution.
Pericardial cysts
Congenital pericardial cysts are uncommon; they may be unilocular or multilocular, with the diameter from 1–5 cm.81Inflammatory cysts comprise pseudocysts as well as encapsulated and loculated pericardial effusions, caused by rheumatic pericarditis, bacterial infection, particularly tuberculosis, trauma and cardiac surgery. Echinococcal cysts usually originate from ruptured hydatid cysts in the liver and lungs. Most patients are asymptomatic and cysts are detected incidentally on chest roentgenograms as an oval, homogeneous radiodense lesion, usually at the right cardiophrenic angle.82 However, the patients can also present with chest discomfort, dyspnoea, cough or palpitations, due to the compression of the heart. Echocardiography is useful, but additional imaging by computed tomography (density readings) or magnetic resonance is often needed.83 The treatment for congenital and inflammatory cysts is percutaneous aspiration and ethanol sclerosis.84,85 If this is not feasible, video assisted thoracotomy or surgical resection may be necessary. The surgical excision of ecchinococcal cysts is not recommended. Percutanous aspiration and instillation of ethanol or silver nitrate after pre-treatment with Albendazole (800 mg/day 4 weeks) is safe and effective.85
Specific forms of pericarditis
Viral pericarditis
Viral pericarditis is the most common infection of the pericardium. Inflammatory abnormalities are due to direct viral attack, the immune response (antiviral or anticardiac), or both.3,86 Early viral replication in pericardial and epimyocardial tissue elicits cellular and humoral immune responses against the virus and/or cardiac tissue. Viral genomic fragments in pericardial tissue may not necessarily replicate, yet they serve as a source of antigen to stimulate immune responses. Deposits of IgM, IgG, and occasionally IgA, can be found in the pericardium and myocardium for years.86 Various viruses cause pericarditis (entero-, echo-, adeno-, cytomegalo-, Ebstein Barr-, herpes simplex-, influenza, parvo B19, hepatitis C, HIV, etc). Attacks of enteroviral pericarditis follow the seasonal epidemics of Coxsackie virus A+B and Echovirus infections.87 Cytomegalovirus pericarditis has an increased incidence in immunocompromised and HIV infected hosts.88 Infectious mononucleosis may also present with pericarditis. The diagnosis of viral pericarditis is not possible without the evaluation of pericardial effusion and/or pericardial/epicardial tissue, preferably by PCR or in-situ hybridisation (level of evidence B, class IIa indication) (Focus boxes 3–4). A four-fold rise in serum antibody levels is suggestive but not diagnostic for viral pericarditis (level of evidence B, class IIb indication).
Treatment of viral pericarditis is directed to resolve symptoms (see acute pericarditis), prevent complications, and eradicate the virus. In patients with chronic or recurrent symptomatic pericardial effusion and confirmed viral infection the following specific treatment is under investigation: (1) CMV pericarditis: hyperimmunoglobulin - 1 time per day 4 ml/kg on day 0, 4, and 8; 2 ml/kg on day 12 and 16; (2) Coxsackie B pericarditis: Interferon alpha or beta 2,5 Mio. IU/m2 surface area s.c. 3×per week; (3) adenovirus and parvovirus B19 perimyocarditis: immunoglobulin treatment: 10 g intravenously at day 1 and 3 for 6–8 hours.113
Pericardial manifestation of human immunodeficiency virus (HIV) infection can be due to infective, non-infective and neoplastic diseases (Kaposi sarcoma and/or lymphoma). Infective (myo)pericarditis results from the local HIV infection and/or from the other viral (cytomegalovirus, herpes simplex), bacterial (S. aureus, K. pneumoniae, M. avium, and M. tuberculosis) and fungal coinfections (Cryptococcus neoformans).114 In progressive disease the incidence of echocardiographically detected pericardial effusion is up to 40%.115 Cardiac tamponade is rare.116 During the treatment with retroviral compounds, lipodystrophy can develop (best demonstrated by MRI) with intense paracardial fat deposition leading to heart failure. Treatment is symptomatic, while in large effusions and cardiac tamponade pericardiocentesis is necessary. The use of corticoid therapy is contraindicated except in patients with secondary tuberculous pericarditis, as an adjunct to tuberculostatic treatment (level of evidence A, indication I).117
Bacterial pericarditis
Purulent pericarditis in adults is rare (Table 5), but always fatal if untreated.118–121 Mortality rate in treated patients is 40%, mostly due to cardiac tamponade, toxicity, and constriction. It is usually a complication of an infection originating elsewhere in the body, arising by contiguous spread or haematogenous dissemination.131 Predisposing conditions are pericardial effusion, immunosuppression, chronic diseases (alcohol abuse, rheumatoid arthritis, etc), cardiac surgery and chest trauma. The disease appears as an acute, fulminant infectious illness with short duration. Percutaneous pericardiocentesis must be promptly performed. Obtained pericardial fluid should undergo urgent Gram, acid-fast and fungal staining, followed by cultures of the pericardial and body fluids (level of evidence B, indication I). Rinsing of the pericardial cavity, combined with effective systemic antibiotic therapy is mandatory (antistaphylococcal antibiotic plus aminoglycoside, followed by tailored antibiotic therapy according to pericardial fluid and blood cultures).119 Intrapericardial instillation of antibiotics (e.g., gentamycin) is useful but not sufficient. Frequent irrigation of the pericardial cavity with urokinase or streptokinase, using large catheters, may liquefy the purulent exudate,120,121 but open surgical drainage through subxiphoid pericardiotomy is preferable.118 Pericardiectomy is required in patients with dense adhesions, loculated and thick purulent effusion, recurrence of tamponade, persistent infection, and progression to constriction.119 Surgical mortality is up to 8%.
Differential diagnosis of the specific forms of pericarditis118–130
Viral | Bacterial | Tuberculous | Autoreactive | |
|---|---|---|---|---|
| Cardiotropic microbial agents | Entero-, echo-, adeno-, cytomegalo, Ebstein Barr, herpes simplex, influenza, parvo B19, hepatitis A,B,C virus, HIV | Staphylococci, pneumococci, streptococci, Neisseria, proteus, gram negative rods, Legionella | Mycobacterium tuberculosis | Autoimmune process in the absence of viral and bacterial agents |
| Etiological evidence by | PCR or in situ hybridisation (evidence level B, indication IIa) | Gram-stain, bacterial culture, PCR for Borrelia and chlamydia pneumoniae (evidence level B, indication I) | Ziehl-Neelsen, auramin 0 stain, culture, PCR (evidence level B, indication I) | Ig-binding to peri- and epicardium, negative PCR for cardiotropic agents, epicarditis (evidence level B, indication IIa) |
| Incidence (%) Western countries | 30 | 5–10 5 per 100,000 patients | \({<}\) 4 (much more in Africa and South America) | 20–30 |
| Male: female ratio | 3:1 | 1:1 | 1:1 | 1:1 |
| Predisposition | Unknown | Chronic alcohol abuse, immuno-suppression, | Alcohol abuse, HIV infection | Association to autoimmune disorders |
| Clinical features | Identical to acute pericarditis, often subfebrile | Spiking fever, fulminant, tachycardia, pericardial rubs | Subfebrile, chronic | Subfebrile, chronic |
| Effusion size | Variable, mostly small | Variable | Variable, mostly large | Variable |
| Tamponade | Infrequent | 80% | Frequent | Infrequent |
| Spontan. Remission | Frequent | None | None | Rare |
| Recurrence rate | 30–50% | Rare | Frequent | Frequent; \(>\) 25% |
| Aspect of PE | Serous/serosanginous | Purulent | Serosanginous | Serous |
| Protein content | \(>\) 3 g/dL | High | High/intermediate | Intermediate |
| Leukocyte count (PE) | \(>\) 5000/ml | ≫10000/ml | Intermediate \(>\) 8000 | Intermediate <5000 |
| Pericardial fluid analyses | Activated lymphocytes and macrophages (sparse) Adenosindeaminase (ADA)- negative | Granulocytes and macrophages (massive) ADA-negative | Granulocytes and macrophages (intermediate) ADA positive ( \(>\) 40 U/ml) | Activated lymphocytes and macrophages (sparse) ADA-negative |
| Peri- and epicardial biopsy | Lymphocytic peri-/epicarditis, PCR positive for cardiotropic virus | Leukocytic epicarditis | Caseous granuloma, PCR | Lymphocytic peri-/epicarditis, PCR negative |
| Mortality if untreated | Depending on agent and tamponade | 100% | 85% | In untreated tamponade |
| Intrapericardial treatment | Drainage, if needed, no intrapercardial corticoids | Drainage and rinsing (saline) gentamycin 80 mg i.p., | Drainage, if needed | Drainage, i.p. triamcinolon (evidence B, indication IIa) |
| Pericardiotomy/pericardiectomy | Rarely needed | Promptly needed (evidence level B, indication I) | Rarely needed | Rarely needed |
| Systemic treatment | I.V. immunoglobulins, IFN (in enteroviral pericarditis) s.c. | I.V. antibiotics | Tuberculostatic+prednisone | NSAIDs, Colchicine, prednisolone/azathioprin |
| Constriction | Rare | Frequent | Frequent (30–50%) | Rare |
Viral | Bacterial | Tuberculous | Autoreactive | |
|---|---|---|---|---|
| Cardiotropic microbial agents | Entero-, echo-, adeno-, cytomegalo, Ebstein Barr, herpes simplex, influenza, parvo B19, hepatitis A,B,C virus, HIV | Staphylococci, pneumococci, streptococci, Neisseria, proteus, gram negative rods, Legionella | Mycobacterium tuberculosis | Autoimmune process in the absence of viral and bacterial agents |
| Etiological evidence by | PCR or in situ hybridisation (evidence level B, indication IIa) | Gram-stain, bacterial culture, PCR for Borrelia and chlamydia pneumoniae (evidence level B, indication I) | Ziehl-Neelsen, auramin 0 stain, culture, PCR (evidence level B, indication I) | Ig-binding to peri- and epicardium, negative PCR for cardiotropic agents, epicarditis (evidence level B, indication IIa) |
| Incidence (%) Western countries | 30 | 5–10 5 per 100,000 patients | \({<}\) 4 (much more in Africa and South America) | 20–30 |
| Male: female ratio | 3:1 | 1:1 | 1:1 | 1:1 |
| Predisposition | Unknown | Chronic alcohol abuse, immuno-suppression, | Alcohol abuse, HIV infection | Association to autoimmune disorders |
| Clinical features | Identical to acute pericarditis, often subfebrile | Spiking fever, fulminant, tachycardia, pericardial rubs | Subfebrile, chronic | Subfebrile, chronic |
| Effusion size | Variable, mostly small | Variable | Variable, mostly large | Variable |
| Tamponade | Infrequent | 80% | Frequent | Infrequent |
| Spontan. Remission | Frequent | None | None | Rare |
| Recurrence rate | 30–50% | Rare | Frequent | Frequent; \(>\) 25% |
| Aspect of PE | Serous/serosanginous | Purulent | Serosanginous | Serous |
| Protein content | \(>\) 3 g/dL | High | High/intermediate | Intermediate |
| Leukocyte count (PE) | \(>\) 5000/ml | ≫10000/ml | Intermediate \(>\) 8000 | Intermediate <5000 |
| Pericardial fluid analyses | Activated lymphocytes and macrophages (sparse) Adenosindeaminase (ADA)- negative | Granulocytes and macrophages (massive) ADA-negative | Granulocytes and macrophages (intermediate) ADA positive ( \(>\) 40 U/ml) | Activated lymphocytes and macrophages (sparse) ADA-negative |
| Peri- and epicardial biopsy | Lymphocytic peri-/epicarditis, PCR positive for cardiotropic virus | Leukocytic epicarditis | Caseous granuloma, PCR | Lymphocytic peri-/epicarditis, PCR negative |
| Mortality if untreated | Depending on agent and tamponade | 100% | 85% | In untreated tamponade |
| Intrapericardial treatment | Drainage, if needed, no intrapercardial corticoids | Drainage and rinsing (saline) gentamycin 80 mg i.p., | Drainage, if needed | Drainage, i.p. triamcinolon (evidence B, indication IIa) |
| Pericardiotomy/pericardiectomy | Rarely needed | Promptly needed (evidence level B, indication I) | Rarely needed | Rarely needed |
| Systemic treatment | I.V. immunoglobulins, IFN (in enteroviral pericarditis) s.c. | I.V. antibiotics | Tuberculostatic+prednisone | NSAIDs, Colchicine, prednisolone/azathioprin |
| Constriction | Rare | Frequent | Frequent (30–50%) | Rare |
Differential diagnosis of the specific forms of pericarditis118–130
Viral | Bacterial | Tuberculous | Autoreactive | |
|---|---|---|---|---|
| Cardiotropic microbial agents | Entero-, echo-, adeno-, cytomegalo, Ebstein Barr, herpes simplex, influenza, parvo B19, hepatitis A,B,C virus, HIV | Staphylococci, pneumococci, streptococci, Neisseria, proteus, gram negative rods, Legionella | Mycobacterium tuberculosis | Autoimmune process in the absence of viral and bacterial agents |
| Etiological evidence by | PCR or in situ hybridisation (evidence level B, indication IIa) | Gram-stain, bacterial culture, PCR for Borrelia and chlamydia pneumoniae (evidence level B, indication I) | Ziehl-Neelsen, auramin 0 stain, culture, PCR (evidence level B, indication I) | Ig-binding to peri- and epicardium, negative PCR for cardiotropic agents, epicarditis (evidence level B, indication IIa) |
| Incidence (%) Western countries | 30 | 5–10 5 per 100,000 patients | \({<}\) 4 (much more in Africa and South America) | 20–30 |
| Male: female ratio | 3:1 | 1:1 | 1:1 | 1:1 |
| Predisposition | Unknown | Chronic alcohol abuse, immuno-suppression, | Alcohol abuse, HIV infection | Association to autoimmune disorders |
| Clinical features | Identical to acute pericarditis, often subfebrile | Spiking fever, fulminant, tachycardia, pericardial rubs | Subfebrile, chronic | Subfebrile, chronic |
| Effusion size | Variable, mostly small | Variable | Variable, mostly large | Variable |
| Tamponade | Infrequent | 80% | Frequent | Infrequent |
| Spontan. Remission | Frequent | None | None | Rare |
| Recurrence rate | 30–50% | Rare | Frequent | Frequent; \(>\) 25% |
| Aspect of PE | Serous/serosanginous | Purulent | Serosanginous | Serous |
| Protein content | \(>\) 3 g/dL | High | High/intermediate | Intermediate |
| Leukocyte count (PE) | \(>\) 5000/ml | ≫10000/ml | Intermediate \(>\) 8000 | Intermediate <5000 |
| Pericardial fluid analyses | Activated lymphocytes and macrophages (sparse) Adenosindeaminase (ADA)- negative | Granulocytes and macrophages (massive) ADA-negative | Granulocytes and macrophages (intermediate) ADA positive ( \(>\) 40 U/ml) | Activated lymphocytes and macrophages (sparse) ADA-negative |
| Peri- and epicardial biopsy | Lymphocytic peri-/epicarditis, PCR positive for cardiotropic virus | Leukocytic epicarditis | Caseous granuloma, PCR | Lymphocytic peri-/epicarditis, PCR negative |
| Mortality if untreated | Depending on agent and tamponade | 100% | 85% | In untreated tamponade |
| Intrapericardial treatment | Drainage, if needed, no intrapercardial corticoids | Drainage and rinsing (saline) gentamycin 80 mg i.p., | Drainage, if needed | Drainage, i.p. triamcinolon (evidence B, indication IIa) |
| Pericardiotomy/pericardiectomy | Rarely needed | Promptly needed (evidence level B, indication I) | Rarely needed | Rarely needed |
| Systemic treatment | I.V. immunoglobulins, IFN (in enteroviral pericarditis) s.c. | I.V. antibiotics | Tuberculostatic+prednisone | NSAIDs, Colchicine, prednisolone/azathioprin |
| Constriction | Rare | Frequent | Frequent (30–50%) | Rare |
Viral | Bacterial | Tuberculous | Autoreactive | |
|---|---|---|---|---|
| Cardiotropic microbial agents | Entero-, echo-, adeno-, cytomegalo, Ebstein Barr, herpes simplex, influenza, parvo B19, hepatitis A,B,C virus, HIV | Staphylococci, pneumococci, streptococci, Neisseria, proteus, gram negative rods, Legionella | Mycobacterium tuberculosis | Autoimmune process in the absence of viral and bacterial agents |
| Etiological evidence by | PCR or in situ hybridisation (evidence level B, indication IIa) | Gram-stain, bacterial culture, PCR for Borrelia and chlamydia pneumoniae (evidence level B, indication I) | Ziehl-Neelsen, auramin 0 stain, culture, PCR (evidence level B, indication I) | Ig-binding to peri- and epicardium, negative PCR for cardiotropic agents, epicarditis (evidence level B, indication IIa) |
| Incidence (%) Western countries | 30 | 5–10 5 per 100,000 patients | \({<}\) 4 (much more in Africa and South America) | 20–30 |
| Male: female ratio | 3:1 | 1:1 | 1:1 | 1:1 |
| Predisposition | Unknown | Chronic alcohol abuse, immuno-suppression, | Alcohol abuse, HIV infection | Association to autoimmune disorders |
| Clinical features | Identical to acute pericarditis, often subfebrile | Spiking fever, fulminant, tachycardia, pericardial rubs | Subfebrile, chronic | Subfebrile, chronic |
| Effusion size | Variable, mostly small | Variable | Variable, mostly large | Variable |
| Tamponade | Infrequent | 80% | Frequent | Infrequent |
| Spontan. Remission | Frequent | None | None | Rare |
| Recurrence rate | 30–50% | Rare | Frequent | Frequent; \(>\) 25% |
| Aspect of PE | Serous/serosanginous | Purulent | Serosanginous | Serous |
| Protein content | \(>\) 3 g/dL | High | High/intermediate | Intermediate |
| Leukocyte count (PE) | \(>\) 5000/ml | ≫10000/ml | Intermediate \(>\) 8000 | Intermediate <5000 |
| Pericardial fluid analyses | Activated lymphocytes and macrophages (sparse) Adenosindeaminase (ADA)- negative | Granulocytes and macrophages (massive) ADA-negative | Granulocytes and macrophages (intermediate) ADA positive ( \(>\) 40 U/ml) | Activated lymphocytes and macrophages (sparse) ADA-negative |
| Peri- and epicardial biopsy | Lymphocytic peri-/epicarditis, PCR positive for cardiotropic virus | Leukocytic epicarditis | Caseous granuloma, PCR | Lymphocytic peri-/epicarditis, PCR negative |
| Mortality if untreated | Depending on agent and tamponade | 100% | 85% | In untreated tamponade |
| Intrapericardial treatment | Drainage, if needed, no intrapercardial corticoids | Drainage and rinsing (saline) gentamycin 80 mg i.p., | Drainage, if needed | Drainage, i.p. triamcinolon (evidence B, indication IIa) |
| Pericardiotomy/pericardiectomy | Rarely needed | Promptly needed (evidence level B, indication I) | Rarely needed | Rarely needed |
| Systemic treatment | I.V. immunoglobulins, IFN (in enteroviral pericarditis) s.c. | I.V. antibiotics | Tuberculostatic+prednisone | NSAIDs, Colchicine, prednisolone/azathioprin |
| Constriction | Rare | Frequent | Frequent (30–50%) | Rare |
Tuberculous pericarditis
In the last decade TBC pericarditis in the developed countries has been primarily seen in immunocompromised patients (AIDS).123 The mortality rate in untreated acute effusive TBC pericarditis approaches 85%. Pericardial constriction occurs in 30–50%.122,125 The clinical presentation is variable: acute pericarditis with or without effusion; cardiac tamponade, silent, often large pericardial effusion with a relapsing course, toxic symptoms with persistent fever, acute constrictive pericarditis, subacute constriction, effusive-constrictive, or chronic constrictive pericarditis, and pericardial calcifications.3,89 The diagnosis is made by the identification of Mycobacterium tuberculosis in the pericardial fluid or tissue, and/or the presence of caseous granulomas in the pericardium.3,123 Importantly, PCR can identify DNA of Mycobacterium tuberculosis rapidly from only 1 μL of pericardial fluid.127,128 High adenosine deaminase activity and interferon gamma concentration in pericardial effusion are also diagnostic, with a high sensitivity and specificity (Focus box 3): Both pericardioscopy and pericardial biopsy have also improved the diagnostic accuracy for TBC pericarditis.15 Pericardial biopsy enables rapid diagnosis with better sensitivity than pericardiocentesis (100 vs. 33%).
Pericarditis in a patient with proven extracardiac tuberculosis is strongly suggestive of TBC aetiology (several sputum cultures should be taken).3,126 The tuberculin skin test may be false negative in 25–33% of tests122 and false positive in 30–40% of patients.123 More accurate enzyme-linked immunospot (ELISPOT) test detects T-cells specific for Mycobacterium tuberculosis antigen.132 Perimyocardial TBC involvement is also associated with high serum titres of antimyolemmal and antimyosin antibodies.133 The diagnostic yield of pericardiocentesis in TBC pericarditis ranges from 30–76% according to the methods applied for the analyses of pericardial effusion.122,127 Pericardial fluid demonstrates high specific gravity, high protein levels, and high white-cell count (from 0.7–54×109/l).123
Various antituberculous drug combinations of different lengths (6, 9, 12 months) have been applied.94,122,123,126 However, only patients with proven or very likely TBC pericarditis should be treated. Prevention of constriction in chronic pericardial effusion of undetermined aetiology by “ex iuvantibus” antitubercular treatment was not successful.134 The use of steroids remains controversial.126,130,135–137 A meta analysis of patients with effusive and constrictive TBC pericarditis136,137 suggested that tuberculostatic treatment combined with steroids might be associated with fewer deaths, less frequent need for pericardiocentesis or pericardiectomy (level of evidence A, indication IIb).126,129 If given, prednisone should be administered in relatively high doses (1–2 mg/kg per day) since rifampicin induces its liver metabolism.7 This dose is maintained for 5–7 days and is progressively reduced to discontinuation in 6–8 weeks. If, in spite of combination therapy, constriction develops pericardiectomy is indicated (level of evidence B, class I indication).
Pericarditis in renal failure
Renal failure is a common cause of pericardial disease, producing large pericardial effusions in up to 20% of patients.138 Two forms have been described: (1) Uremic pericarditis – in 6–10% of patients with advanced renal failure (acute or chronic) before dialysis has been instituted or shortly thereafter.139 It results from inflammation of the visceral and parietal pericardium and correlates with the degree of azotemia (BUN
Most patients with uremic pericarditis respond rapidly to haemo- or peritoneal dialysis with resolution of chest pain and pericardial effusion. To avoid haemopericardium heparin-free haemodialysis should be used. Hypokalemia and hypophosphatemia should be prevented by supplementing the dialysis solution when appropriate.144 Intensified dialysis usually leads to resolution of the pericarditis within 1–2 weeks.145 Peritoneal dialysis, which does not require heparinisation, may be therapeutic in pericarditis resistant to haemodialysis, or if heparin-free haemodialysis cannot be performed. NSAIDs and systemic corticosteroids have limited success when intensive dialysis is ineffective.146 Cardiac tamponade and large chronic effusions resistant to dialysis must be treated with pericardiocentesis. (level of evidence B, class IIa indication). Large, non-resolving symptomatic effusions should be treated with intrapericardial instillation of corticosteroids after pericardiocentesis or subxiphoid pericardiotomy (triamcinolone hexacetonide 50 mg every 6 h for 2–3 days).140,147 Pericardiectomy is indicated only in refractory, severely symptomatic patients due to its potential morbidity and mortality. After renal transplantation, pericarditis has also been reported in 2.4% of patients, within two months.148 Uraemia or infection (CMV) may be the causes.
Autoreactive pericarditis and pericardial involvement in systemic autoimmune diseases
The diagnosis of autoreactive pericarditis is established using the following criteria:2 (1) increased number of lymphocytes and mononuclear cells
Pericarditis occurs in systemic autoimmune diseases: rheumatoid arthritis, systemic lupus erythematosus, progressive systemic sclerosis, polymyositis/ dermatomyositis, mixed connective tissue disease, seronegative spondyloarthropathies, systemic and hypersensitivity vasculitides, Behçet syndrome, Wegener granulomatosis, and sarcoidosis.7 Intensified treatment of the underlying disease and symptomatic management are indicated (evidence level B, indication I).
The post-cardiac injury syndrome: postpericardiotomy syndrome
Post-cardiac injury syndrome develops within days to months after cardiac, pericardial injury or both.7,149 It resembles the post-myocardial infarction syndrome, both appearing to be variants of a common immunopathic process. Unlike post-myocardial infarction syndrome, post-cardiac injury syndrome acutely provokes a greater antiheart antibody response (antisarcolemmal and antifibrillary), probably related to more extensive release of antigenic material.149,150 Pericardial effusion also occurs after orthotopic heart transplantation (21%). It is more frequent in patients receiving aminocaproic acid during the operation.151 Cardiac tamponade after open heart surgery is more common following valve surgery than coronary artery bypass grafting (CABG) alone and may be related to the preoperative use of anticoagulants.152 Constrictive pericarditis may also occur after cardiac surgery. Warfarin administration in patients with early postoperative pericardial effusion imposes the greatest risk, particularly in those who did not undergo pericardiocentesis and drainage of the effusion.153 Symptomatic treatment is as in acute pericarditis (NSAIDs or colchicine for several weeks or months, even after disappearance of effusion).154 Long term (3–6 months) oral corticoids or preferably pericardiocentesis and intrapericardial instillation of triamcinolone (300 mg/m2) are therapeutic options in refractory forms. Redo surgery and pericardiectomy are very rarely needed. Primary prevention of postperiocardiotomy syndrome using short-term perioperative steroid treatment or colchicine is under investigation.155
Postinfarction pericarditis
Two forms of postinfarction pericarditis can be distinguished: an “early” form (pericarditis epistenocardica) and a “delayed” form (Dressler's syndrome).156Epistenocardiac pericarditis, caused by direct exudation, occurs in 5–20% of transmural myocardial infarctions but is clinically discovered rarely. Dressler's syndrome occurs from one week to several months after clinical onset of myocardial infarction with symptoms and manifestations similar to the post-cardiac injury syndrome. It does not require transmural infarction157 and can also appear as an extension of epistenocardiac pericarditis. Its incidence is 0.5–5%158 and is still lower in patients treated with thrombolytics (
Hospitalisation to observe for tamponade, differential diagnosis, and adjustments of treatment is needed. Ibuprofen, which increases coronary flow, is the agent of choice.165 Aspirin, up to 650 mg every 4 hours for 2 to 5 days has also been successfully applied. Other nonsteroidal agents risk thinning the infarction zone.164,166 Corticosteroid therapy can be used for refractory symptoms only but could delay myocardial infarction healing (level of evidence B, class IIa indication).7
Traumatic pericardial effusion and haemopericardium in aortic dissection
Direct pericardial injury can be induced by accidents or iatrogenic wounds.7,167–170 Blood loss, vasoconstriction, and haematothorax leading to severe hypotension and shock may mask pulses paradoxus.170 Thoracotomy and surgical repair should be performed.
Iatrogenic tamponade occurs most frequently in percutaneous mitral valvuloplasty, during or after transseptal puncture, particularly, if no biplane catheterisation laboratory is available and a small left atrium is present. Whereas the puncture of the interatrial septum is asymptomatic, the passage of the free wall induces chest-pain immediately. If high-pressure containing structures are punctured, rapid deterioration occurs. However, if only the atrial wall is passed, the onset of symptoms and the tamponade may be delayed for 4 to 6 hours. Rescue pericardiocentesis is successful in 95–100% with a
Traumatic pericardial effusion167–194
Effusion due to | Incidence (%) | Mortality (%) | Management | Comment/Reference | ||||
|---|---|---|---|---|---|---|---|---|
| Iatrogenic | ||||||||
| Transseptal puncture | 1–3 | \({<}\) 1% | Rescue pericardiocentesis, if needed | Use biplane angio-graphy171 | ||||
| Coronary artery perforation during PTCA (guidewire only) | Not infrequent | Not available | Watchful waiting by withdrawal of guidewire | Reverse anticoagulation | ||||
| Coronary artery transsection during PTCA | 0.3–3.2 | Not available | Sealing by graft stents (best) or perfusion catheters with balloon occlusion of perforated vessel, if pericardial puncture is need reinfusion of recovered blood in vein avoids anaemia. | Surgery only if \(>\) 30% of myocardium at stake or bleeding cannot be stopped172,173 | ||||
| Rotablation | 0.1–3 | Not available | See above | See above172,173 | ||||
| Transluminal extraction atherectomy (atherocath) | 0–2 % | Not available | See above | See above | ||||
| Excimer laser angioplasty | 1.7–3% | Not available | See above | See above173 | ||||
| High pressure stenting | \({<}\) 2% (?) | Not available | See above | See above173 | ||||
| Mitral valvuloplasty | 1–3% | <1% | 171,179 | |||||
| Left ventricular biopsy (LV-EMB) | 0.1–3.3% | 0% | Routine echocardiography post EMB, pericardiocentesis, if needed; reverse anticoagulation | 180,181,194 | ||||
| Right ventricular biopsy (RV-EMB) | 0.3–5% | 0–0.05% | Routine echocardiography post EMB, pericardiocentesis, if needed; reverse anticoagulation | 180,181,194 | ||||
| Pacemaker leads | 0–3–3.1% | 0.1% | Routine echocardiography post implantation, pericardiocentesis, if needed | Pericardial effusion with/without tamponade190,191, postpericardiotomy syndrome192, constrictive pericarditis193 | ||||
| Other causes | ||||||||
| Injury (direct: e.g., stabbing indirect: compression, closed chest massage) | Not available | Often lethal | Direct: surgery (see text) Indirect: pericardiocentesis or surgery | |||||
| Aortic dissection | 48% post mortem, 17–45% in clinical series | Lethal if not operated | Transoesophageal echo, CT or MRI, immediate surgery | Particularly in De- Bakey I + II=Stanford type A184–189 | ||||
Effusion due to | Incidence (%) | Mortality (%) | Management | Comment/Reference | ||||
|---|---|---|---|---|---|---|---|---|
| Iatrogenic | ||||||||
| Transseptal puncture | 1–3 | \({<}\) 1% | Rescue pericardiocentesis, if needed | Use biplane angio-graphy171 | ||||
| Coronary artery perforation during PTCA (guidewire only) | Not infrequent | Not available | Watchful waiting by withdrawal of guidewire | Reverse anticoagulation | ||||
| Coronary artery transsection during PTCA | 0.3–3.2 | Not available | Sealing by graft stents (best) or perfusion catheters with balloon occlusion of perforated vessel, if pericardial puncture is need reinfusion of recovered blood in vein avoids anaemia. | Surgery only if \(>\) 30% of myocardium at stake or bleeding cannot be stopped172,173 | ||||
| Rotablation | 0.1–3 | Not available | See above | See above172,173 | ||||
| Transluminal extraction atherectomy (atherocath) | 0–2 % | Not available | See above | See above | ||||
| Excimer laser angioplasty | 1.7–3% | Not available | See above | See above173 | ||||
| High pressure stenting | \({<}\) 2% (?) | Not available | See above | See above173 | ||||
| Mitral valvuloplasty | 1–3% | <1% | 171,179 | |||||
| Left ventricular biopsy (LV-EMB) | 0.1–3.3% | 0% | Routine echocardiography post EMB, pericardiocentesis, if needed; reverse anticoagulation | 180,181,194 | ||||
| Right ventricular biopsy (RV-EMB) | 0.3–5% | 0–0.05% | Routine echocardiography post EMB, pericardiocentesis, if needed; reverse anticoagulation | 180,181,194 | ||||
| Pacemaker leads | 0–3–3.1% | 0.1% | Routine echocardiography post implantation, pericardiocentesis, if needed | Pericardial effusion with/without tamponade190,191, postpericardiotomy syndrome192, constrictive pericarditis193 | ||||
| Other causes | ||||||||
| Injury (direct: e.g., stabbing indirect: compression, closed chest massage) | Not available | Often lethal | Direct: surgery (see text) Indirect: pericardiocentesis or surgery | |||||
| Aortic dissection | 48% post mortem, 17–45% in clinical series | Lethal if not operated | Transoesophageal echo, CT or MRI, immediate surgery | Particularly in De- Bakey I + II=Stanford type A184–189 | ||||
Traumatic pericardial effusion167–194
Effusion due to | Incidence (%) | Mortality (%) | Management | Comment/Reference | ||||
|---|---|---|---|---|---|---|---|---|
| Iatrogenic | ||||||||
| Transseptal puncture | 1–3 | \({<}\) 1% | Rescue pericardiocentesis, if needed | Use biplane angio-graphy171 | ||||
| Coronary artery perforation during PTCA (guidewire only) | Not infrequent | Not available | Watchful waiting by withdrawal of guidewire | Reverse anticoagulation | ||||
| Coronary artery transsection during PTCA | 0.3–3.2 | Not available | Sealing by graft stents (best) or perfusion catheters with balloon occlusion of perforated vessel, if pericardial puncture is need reinfusion of recovered blood in vein avoids anaemia. | Surgery only if \(>\) 30% of myocardium at stake or bleeding cannot be stopped172,173 | ||||
| Rotablation | 0.1–3 | Not available | See above | See above172,173 | ||||
| Transluminal extraction atherectomy (atherocath) | 0–2 % | Not available | See above | See above | ||||
| Excimer laser angioplasty | 1.7–3% | Not available | See above | See above173 | ||||
| High pressure stenting | \({<}\) 2% (?) | Not available | See above | See above173 | ||||
| Mitral valvuloplasty | 1–3% | <1% | 171,179 | |||||
| Left ventricular biopsy (LV-EMB) | 0.1–3.3% | 0% | Routine echocardiography post EMB, pericardiocentesis, if needed; reverse anticoagulation | 180,181,194 | ||||
| Right ventricular biopsy (RV-EMB) | 0.3–5% | 0–0.05% | Routine echocardiography post EMB, pericardiocentesis, if needed; reverse anticoagulation | 180,181,194 | ||||
| Pacemaker leads | 0–3–3.1% | 0.1% | Routine echocardiography post implantation, pericardiocentesis, if needed | Pericardial effusion with/without tamponade190,191, postpericardiotomy syndrome192, constrictive pericarditis193 | ||||
| Other causes | ||||||||
| Injury (direct: e.g., stabbing indirect: compression, closed chest massage) | Not available | Often lethal | Direct: surgery (see text) Indirect: pericardiocentesis or surgery | |||||
| Aortic dissection | 48% post mortem, 17–45% in clinical series | Lethal if not operated | Transoesophageal echo, CT or MRI, immediate surgery | Particularly in De- Bakey I + II=Stanford type A184–189 | ||||
Effusion due to | Incidence (%) | Mortality (%) | Management | Comment/Reference | ||||
|---|---|---|---|---|---|---|---|---|
| Iatrogenic | ||||||||
| Transseptal puncture | 1–3 | \({<}\) 1% | Rescue pericardiocentesis, if needed | Use biplane angio-graphy171 | ||||
| Coronary artery perforation during PTCA (guidewire only) | Not infrequent | Not available | Watchful waiting by withdrawal of guidewire | Reverse anticoagulation | ||||
| Coronary artery transsection during PTCA | 0.3–3.2 | Not available | Sealing by graft stents (best) or perfusion catheters with balloon occlusion of perforated vessel, if pericardial puncture is need reinfusion of recovered blood in vein avoids anaemia. | Surgery only if \(>\) 30% of myocardium at stake or bleeding cannot be stopped172,173 | ||||
| Rotablation | 0.1–3 | Not available | See above | See above172,173 | ||||
| Transluminal extraction atherectomy (atherocath) | 0–2 % | Not available | See above | See above | ||||
| Excimer laser angioplasty | 1.7–3% | Not available | See above | See above173 | ||||
| High pressure stenting | \({<}\) 2% (?) | Not available | See above | See above173 | ||||
| Mitral valvuloplasty | 1–3% | <1% | 171,179 | |||||
| Left ventricular biopsy (LV-EMB) | 0.1–3.3% | 0% | Routine echocardiography post EMB, pericardiocentesis, if needed; reverse anticoagulation | 180,181,194 | ||||
| Right ventricular biopsy (RV-EMB) | 0.3–5% | 0–0.05% | Routine echocardiography post EMB, pericardiocentesis, if needed; reverse anticoagulation | 180,181,194 | ||||
| Pacemaker leads | 0–3–3.1% | 0.1% | Routine echocardiography post implantation, pericardiocentesis, if needed | Pericardial effusion with/without tamponade190,191, postpericardiotomy syndrome192, constrictive pericarditis193 | ||||
| Other causes | ||||||||
| Injury (direct: e.g., stabbing indirect: compression, closed chest massage) | Not available | Often lethal | Direct: surgery (see text) Indirect: pericardiocentesis or surgery | |||||
| Aortic dissection | 48% post mortem, 17–45% in clinical series | Lethal if not operated | Transoesophageal echo, CT or MRI, immediate surgery | Particularly in De- Bakey I + II=Stanford type A184–189 | ||||
Transsection of the coronary artery and acute or subacute cardiac tamponade may occur during percutaneous coronary interventions.172,173 A breakthrough in the treatment of coronary perforation is membrane-covered graft stents.177,178 Perforation of the coronary artery by a guidewire is not infrequent and causes very rarely a relevant pericardial haemorrhage.
During right ventricular endomyocardial biopsy, due to the low stiffness of the myocardium, the catheter may pass the myocardium, particularly, when the bioptome has not been opened before reaching the endocardial border. The rate of perforation is reported to be in the range of 0.3–5%, leading to tamponade and circulatory collapse in less than half of the cases.180,181,194 The incidence of pericardial haemorrhage in left ventricular endomyocardial biopsy is lower (0.1–3.3%). Frank cardiac perforations seem to be accompanied by sudden bradycardia and hypotension.180 Severe complications, leading to procedure related mortality were reported in only 0.05% in a worldwide survey of more than 6000 cases181 and in none of the 2537 patients from the registry of an experienced reference centre.194
Pacemaker leads penetrating the right ventricle or epicardial electrodes may cause pericarditis with tamponade, adhesions, or constriction.190–193 A right bundle brand block instead of a usually induced left bundle branch block is a clue.
Blunt chest trauma is the major risk of car accidence. The deceleration force can lead to myocardial contusion with intrapericardial haemorrhage, cardiac rupture, pericardial rupture, or herniation. Transesophageal echocardiography in the emergency room183 or immediate computed tomography should be performed. Pericardial laceration and partial extrusion of the heart into the mediastinum and pleural space may also occur after injury.168
In dissection of the ascending aorta (pericardial effusion can be found in 17–45% of the patients and in 48% of the autopsy cases (Table 6).184 In a clinical series of aortic dissection, pericardial tamponade was found by CT,185 MRI,186 or echocardiography187 in 17–33% of patients with type I dissection and 18–45% in type II dissection and 6% in type III dissection.185 Pericardiocentesis is contraindicated, due to the risk of intensified bleeding and extension of the dissection.188,195 Surgery should be performed immediately (evidence level B, indication I).
Neoplastic pericarditis
Primary tumours of the pericardium are 40 times less common than the metastatic ones.7 Mesothelioma, the most common of the primary tumours, is almost always incurable. The most common secondary malignant tumours are lung cancer, breast cancer, malignant melanoma, lymphomas, and leukemias. Effusions may be small or large with an imminent tamponade (frequent recurrences) or constriction. It even may be the initial sign of malignant disease.196 With small malignant effusions most patients are asymptomatic. The onset of dyspnoea, cough, chest pain, tachycardia, jugular venous distension is observed when the volume of fluid exceeds 500 ml. Pulsus paradoxus, hypotension, cardiogenic shock and paradoxical movement of the jugular venous pulse are important signs of cardiac tamponade. The diagnosis is based on the confirmation of the malignant infiltration within the pericardium. Of note, in almost 2/3 of the patients with documented malignancy pericardial effusion is caused by non-malignant diseases, e.g., radiation pericarditis, or opportunistic infections.102,103 The chest roentgenogram, CT, and MRI may reveal mediastinal widening, hilar masses, and pleural effusion.7 The analyses of pericardial fluid, pericardial or epicardial biopsy are essential for the confirmation of malignant pericardial disease (level of evidence B, indication I) (Focus boxes 3–4).
Treatment of cardiac tamponade is a class I indication for pericardiocentesis. The following steps are recommended in suspected neoplastic pericardial effusion without tamponade: (1) systemic antineoplastic treatment as baseline therapy which can prevent recurrences in up to 67% of cases196 (level of evidence B, class I indication); (2) pericardiocentesis to relieve symptoms and establish diagnosis (level of evidence B, class IIa indication); (3) intrapericardial instillation of cytostatic/sclerosing agent (level of evidence B, class IIa indication). Pericardial drainage is recommended, in all patients with large effusions because of the high recurrence rate (40–70%)(level of evidence B, indication I).197–203 Prevention of recurrences may be achieved by intrapericardial instillation of sclerosing, cytotoxic agents, or immunomodulators. Intrapericardial treatment tailored to the type of the tumour indicates that administration of cisplatin is most effective in secondary lung cancer and intrapericardial instillation of thiotepa was more effective in breast cancer pericardial metastases.204–206 No patient showed signs of constrictive pericarditis (for both agents level of evidence B, indication IIa). Tetracyclines as sclerosing agents also control the malignant pericardial effusion in around 85% of cases, but side effects and complications are quite frequent: fever (19%), chest pain (20%), and atrial arrhythmias (10%) (level of evidence B, indication IIb).196,202,203 Although classic sclerotherapy after intrapericardial instillation of tetracycline, doxycycline, minocycline and bleomycin is an effective procedure, constrictive pericarditis secondary to fibrosis remains a severe problem in long-term survivors.203
Although intrapericardial administration of radionuclides has yielded very good results, it is not widely accepted because of the logistic problems connected with their radioactivity207 (level of evidence B, indication IIa). Radiation therapy is very effective (93%) in controlling malignant pericardial effusion (level of evidence B, indication IIa) in patients with radiosensitive tumours such as lymphomas and leukemias. However, radiotherapy of the heart can cause myocarditis and pericarditis by itself.196 Subxyphoid pericardiotomy is indicated when pericardiocentesis cannot be performed (level of evidence B, indication IIb).208 The procedure can be carried out in local anaesthesia, but complications include myocardial laceration, pneumothorax, and mortality.196,209–213 Pleuropericardiotomy allows drainage of malignant pericardial fluid into the pleural space (level of evidence C, indication IIb). It is associated with a higher complications rate and offers no advantage over pericardiocentesis or subxyphoid pericardiotomy. Pericardiectomy is rarely indicated, mainly for pericardial constriction or complications of previous procedures.196
Percutaneous balloon pericardiotomy creates a pleuro-pericardial direct communication, which allows fluid drainage into the pleural space (level of evidence B, indication IIa). In large malignant pericardial effusions and recurrent tamponade, it seems to be effective (90–97%) and safe.31,214
Rare forms of pericardial disease
Fungal pericarditis
Fungal pericarditis occurs mainly in immunocompromised patients or in the course of endemic-acquired fungal infections.215 The clinical picture comprises the full spectrum of pericardial diseases including fungal myocarditis.3 Fungal pericarditis is mainly due to endemic fungi (Histoplasma, Coccidioides), or nonendemic – opportunistic fungi (Candida, Aspergillus, Blastomyces) and semifungi (Nocardia, Actinomyces).216–218 Diagnosis is obtained by staining and culturing pericardial fluid or tissue. Antifungal antibodies in serum are also helpful in establishing the diagnosis of fungal infection.3 Antifungal treatment with fluconazole, ketoconasole, itraconasole, amphotericin B, liposomal amphotericin B or amphotericin B lipid complex is indicated (level of evidence B, indication I). Corticosteroids and NSAIDs can support the treatment with antifungal drugs (level of evidence C, indication IIa). Patients with pericarditis in the course of histoplasmosis do not need antifungal therapy, but respond to nonsteroidal anti-inflammatory drugs given during 2–12 weeks. Sulfonamides are the drugs of choice for a nocardiosis infection. Combination of three antibiotics including penicillin should be given for actinomycosis (level of evidence C, indication I). Pericardiocentesis or surgical treatment is indicated for haemodynamic impairment. Pericardiectomy is indicated in fungal constrictive pericarditis (evidence level C, indication I).
Radiation pericarditis
The probability to develop radiation-induced pericarditis is influenced by the applied source, dose, its fractionation, duration, radiation exposed volume, form of mantel field therapy, and the age of the patients.219 Radiation induced pericarditis may occur already during the therapy or months and years later – with latency of up to 15–20 years. The effusion may be serous or haemorrhagic, later on with fibrinous adhesions or constriction, typically without tissue calcification. The symptoms may be masked by the underlying disease or the applied chemotherapy. Imaging should start with echocardiography, followed by cardiac CT or MRI if necessary. Pericarditis without tamponade may be treated conservatively or by pericardiocentesis for diagnostic purposes or if haemodynamic compromise/tamponade occurs. Pericardial constriction may happen in up to 20% of patients, requiring pericardiectomy. The operative mortality is high (21%) and the postoperative five years survival rate is very low (1%)220 mostly due to myocardial fibrosis.
Chylopericardium
Chylopericardium refers to a communication between the pericardial sac and the thoracic duct, as a result of trauma, congenital anomalies, or as a complication of open-heart surgery,221 mediastinal lymphangiomas, lymphangiomatous hamartomas, lymphangiectasis, and obstruction or anomalies of the thoracic duct.222 Infection, tamponade or constriction may aggravate the prognosis.223 The pericardial fluid is sterile, odourless, and opalescent with a milky white appearance and the microscopic finding of fat droplets. The chylous nature of the fluid is confirmed by its alkaline reaction, specific gravity between 1010 and 1021,224,225 Sudan III stain for fat, the high concentrations of triglycerides (5–50 g/l) and protein (22–60 g/l). Enhanced computed tomography,226 alone or combined with lymphography, can identify not only the location of the thoracic duct but also its lymphatic connection to the pericardium.227 Treatment depends on the aetiology and the amount of chylous accumulation.228 Chylopericardium after thoracic or cardiac operation is preferably treated by pericardiocentesis and diet (medium chain triglycerides).229,230 If further production of chylous effusion continues, surgical treatment is mandatory (level of evidence B, indication I). When conservative treatment and pericardiocentesis fail, pericardio-peritoneal window is a reasonable option.231,232 Alternatively, when the course of the thoracic duct was precisely identified, its ligation and resection just above the diaphragm is the most effective treatment.233 In secondary chylopericardium the underlying disease should be treated.
Drug- and toxin-related pericarditis
Pericardial reactions to drugs are rare. However, several medications and toxic substances can induce pericarditis, tamponade, adhesions, fibrosis, or constriction (Table 7).7,234 Mechanisms include drug induced lupus reactions, idiosyncrasy, “serum sickness”, foreign substance reactions, and immunopathy. Management is based on the discontinuation of the causative agent and symptomatic treatment.
Drug- and toxin-related pericardial disease7,234
A. Drug-induced lupus erythematosus | ||||
| Procainamide | Methyldopa | Isoniazid | ||
| Tocainide | Mesalazine | Hydantoins | ||
| Hydralazine | Reserpine | |||
| B. Hypersensitivity reaction | ||||
| Penicillins | Tryptophan | Cromolyn sodium | ||
| C. Idiosyncratic reaction or hypersensitivity | ||||
| Methysergide | Amiodarone | Cyclophosphamide | ||
| Minoxidil | Streptokinase | Cyclosporine | ||
| Practolol | p-Aminosalicylic acid | Mesalazine | ||
| Bromocriptine | Thiazides | 5-Fluorouracil | ||
| Psicofuranine | Streptomycin | Vaccines (Smallpox, Yellow fever) | ||
| Polymer fume inhalation | Thiouracils | GM-CSF | ||
| Cytarabine | Sulfa drugs | |||
| Phenylbutazone | ||||
| D. Anthracycline derivatives | ||||
| Doxorubicin | Daunorubicin | |||
| E. Serum sickness | ||||
| Foreign antisera (e.g., antitetanus) | Blood products | |||
| F. Venom | ||||
| Scorpion fish sting | ||||
| G. Foreign-substance reactions (direct pericardial application) | ||||
| Talc (Mg silicate) | Tetracycline/other sclerosants | Iron in β-thalasssemia | ||
| Silicones | Asbestos | |||
| H. Secondary pericardial bleeding/haemopericardium | ||||
| Anticoagulants | Thrombolytic agents | |||
| I. Polymer fume fever – inhalation of the burning fumes of polytetrafluoroethylene (Teflon) | ||||
A. Drug-induced lupus erythematosus | ||||
| Procainamide | Methyldopa | Isoniazid | ||
| Tocainide | Mesalazine | Hydantoins | ||
| Hydralazine | Reserpine | |||
| B. Hypersensitivity reaction | ||||
| Penicillins | Tryptophan | Cromolyn sodium | ||
| C. Idiosyncratic reaction or hypersensitivity | ||||
| Methysergide | Amiodarone | Cyclophosphamide | ||
| Minoxidil | Streptokinase | Cyclosporine | ||
| Practolol | p-Aminosalicylic acid | Mesalazine | ||
| Bromocriptine | Thiazides | 5-Fluorouracil | ||
| Psicofuranine | Streptomycin | Vaccines (Smallpox, Yellow fever) | ||
| Polymer fume inhalation | Thiouracils | GM-CSF | ||
| Cytarabine | Sulfa drugs | |||
| Phenylbutazone | ||||
| D. Anthracycline derivatives | ||||
| Doxorubicin | Daunorubicin | |||
| E. Serum sickness | ||||
| Foreign antisera (e.g., antitetanus) | Blood products | |||
| F. Venom | ||||
| Scorpion fish sting | ||||
| G. Foreign-substance reactions (direct pericardial application) | ||||
| Talc (Mg silicate) | Tetracycline/other sclerosants | Iron in β-thalasssemia | ||
| Silicones | Asbestos | |||
| H. Secondary pericardial bleeding/haemopericardium | ||||
| Anticoagulants | Thrombolytic agents | |||
| I. Polymer fume fever – inhalation of the burning fumes of polytetrafluoroethylene (Teflon) | ||||
Drug- and toxin-related pericardial disease7,234
A. Drug-induced lupus erythematosus | ||||
| Procainamide | Methyldopa | Isoniazid | ||
| Tocainide | Mesalazine | Hydantoins | ||
| Hydralazine | Reserpine | |||
| B. Hypersensitivity reaction | ||||
| Penicillins | Tryptophan | Cromolyn sodium | ||
| C. Idiosyncratic reaction or hypersensitivity | ||||
| Methysergide | Amiodarone | Cyclophosphamide | ||
| Minoxidil | Streptokinase | Cyclosporine | ||
| Practolol | p-Aminosalicylic acid | Mesalazine | ||
| Bromocriptine | Thiazides | 5-Fluorouracil | ||
| Psicofuranine | Streptomycin | Vaccines (Smallpox, Yellow fever) | ||
| Polymer fume inhalation | Thiouracils | GM-CSF | ||
| Cytarabine | Sulfa drugs | |||
| Phenylbutazone | ||||
| D. Anthracycline derivatives | ||||
| Doxorubicin | Daunorubicin | |||
| E. Serum sickness | ||||
| Foreign antisera (e.g., antitetanus) | Blood products | |||
| F. Venom | ||||
| Scorpion fish sting | ||||
| G. Foreign-substance reactions (direct pericardial application) | ||||
| Talc (Mg silicate) | Tetracycline/other sclerosants | Iron in β-thalasssemia | ||
| Silicones | Asbestos | |||
| H. Secondary pericardial bleeding/haemopericardium | ||||
| Anticoagulants | Thrombolytic agents | |||
| I. Polymer fume fever – inhalation of the burning fumes of polytetrafluoroethylene (Teflon) | ||||
A. Drug-induced lupus erythematosus | ||||
| Procainamide | Methyldopa | Isoniazid | ||
| Tocainide | Mesalazine | Hydantoins | ||
| Hydralazine | Reserpine | |||
| B. Hypersensitivity reaction | ||||
| Penicillins | Tryptophan | Cromolyn sodium | ||
| C. Idiosyncratic reaction or hypersensitivity | ||||
| Methysergide | Amiodarone | Cyclophosphamide | ||
| Minoxidil | Streptokinase | Cyclosporine | ||
| Practolol | p-Aminosalicylic acid | Mesalazine | ||
| Bromocriptine | Thiazides | 5-Fluorouracil | ||
| Psicofuranine | Streptomycin | Vaccines (Smallpox, Yellow fever) | ||
| Polymer fume inhalation | Thiouracils | GM-CSF | ||
| Cytarabine | Sulfa drugs | |||
| Phenylbutazone | ||||
| D. Anthracycline derivatives | ||||
| Doxorubicin | Daunorubicin | |||
| E. Serum sickness | ||||
| Foreign antisera (e.g., antitetanus) | Blood products | |||
| F. Venom | ||||
| Scorpion fish sting | ||||
| G. Foreign-substance reactions (direct pericardial application) | ||||
| Talc (Mg silicate) | Tetracycline/other sclerosants | Iron in β-thalasssemia | ||
| Silicones | Asbestos | |||
| H. Secondary pericardial bleeding/haemopericardium | ||||
| Anticoagulants | Thrombolytic agents | |||
| I. Polymer fume fever – inhalation of the burning fumes of polytetrafluoroethylene (Teflon) | ||||
Pericardial effusion in thyroid disorders
Pericardial effusion occurs in 5–30% of patients with hypothyroidism.7 Fluid accumulates slowly and tamponade occurs rarely. In some cases cholesterol pericarditis may be observed. The diagnosis of hypothyroidism is based on serum levels of thyroxin and thyroid stimulating hormone. Bradycardia, low-voltage of the QRS and T wave inversion or flattening in the ECG, cardiomegaly in the roentgenogram and pericardial effusion in echocardiography, as well as a history of radiation induced thyroid dysfunction,235 myopathy, ascites, pleural effusion and uveal oedema may be observed.235–239 Therapy with thyroid hormone decreases pericardial effusion (level of evidence B, indication I).
Pericardial effusion in pregnancy
There is no evidence that pregnancy affects susceptibility to pericardial disease. However, many pregnant women develop a minimal to moderate clinically silent hydropericardium by the third trimester. Cardiac compression is rare.240 ECG changes of acute pericarditis in pregnancy should be distinguished from the slight ST-segment depressions and T-wave changes seen in normal pregnancy.240–241 Occult constriction becomes manifest in pregnancy due to the increased blood volume.241 Most pericardial disorders are managed as in nonpregnant.242,243 Caution is necessary while high-dose aspirin may prematurely close the ductus arteriosus, and colchicine is contraindicated in pregnancy. Pericardiotomy and pericardiectomy can be safely performed if necessary and do not impose a risk for subsequent pregnancies.243,244 Foetal pericardial fluid can be detected by echocardiography after 20 weeks' gestation and is normally 2 mm or less in depth. More fluid should raise questions of hydrops foetalis, Rh disease, hypoalbuminemia, and immunopathy or maternally transmitted mycoplasmal or other infections, and neoplasia.245
Pericardiocentesis is life saving in cardiac tamponade (level of evidence B, class I indication) and indicated in effusions
Pericardiocentesis guided by fluoroscopy is performed in the cardiac catheterisation laboratory with ECG monitoring. Direct ECG monitoring from the puncturing needle is not an adequate safeguard. Right-heart catheterisation can be performed simultaneously, allowing exclusion of constriction. It is prudent to drain the fluid in
Echocardiographic guidance of pericardiocentesis is technically less demanding and can be performed at the bedside.13 Echocardiography should identify the shortest route where the pericardium can be entered intercostally (usually in the sixth or seventh rib space in the anterior axillary line). Prolonged pericardial drainage is performed until the volume of effusion obtained by intermittent pericardial aspiration (every 4–6 h) fall to
The most serious complications of pericardiocentesis are laceration and perforation of the myocardium and the coronary vessels. In addition, patients can experience air embolism, pneumothorax, arrhythmias (usually vasovagal bradycardia), and puncture of the peritoneal cavity or abdominal viscera.26 Internal mammary artery fistulas, acute pulmonary oedema, and purulent pericarditis were rarely reported. The safety was improved with echocardiographic or fluoroscopic guidance. Recent large echocardiographic series reported an incidence of major complications of 1.3–1.6%.13,25,28,29 In fluoroscopy-guided percutaneous pericardiocenteses30 cardiac perforations occurred in 0.9%, serious arrhythmias in 0.6%, arterial bleeding in 1.1%, pneumothorax in 0.6%, infection in 0.3%, and a major vagal reaction in 0.3%. Incidence of major complications was further reduced by utilizing the epicardial halo phenomenon for fluoroscopic guidance.27
Pulsus paradoxus is defined as a drop in systolic blood pressure
Analyses of pericardial effusion can establish the diagnosis of viral, bacterial, tuberculous, fungal, cholesterol, and malignant pericarditis.7 It should be ordered according to the clinical presentation. Cytology and tumour markers (carcinoembryonic antigen (CEA), alpha-feto protein (AFP), carbohydrate antigens CA 125, CA 72-4, CA 15-3, CA 19-9, CD-30, CD-25, etc.) should be performed in suspected malignant disease. In suspected tuberculosis acid-fast bacilli staining, mycobacterium culture or radiometric growth detection (e.g., BACTEC-460), adenosine deaminase (ADA), interferon (IFN)-gamma, pericardial lysozyme, and as well as PCR analyses for tuberculosis should be performed (indication I, level of evidence B).11,89–100 Differentiation of tuberculous and neoplastic effusion is virtually absolute with low levels of ADA and high levels of CEA.94 In addition, very high ADA levels have prognostic value for pericardial constriction.95 However, it should be noted that PCR is as sensitive (75% vs. 83%), but more specific (100% vs. 78%) than ADA estimation for tuberculous pericarditis.99 In suspected bacterial infection at least three cultures of pericardial fluid for aerobes and anaerobes as well as the blood cultures are mandatory (level of evidence B, indication I). PCR analyses for cardiotropic viruses discriminate viral from autoreactive pericarditis (indication IIa, level of evidence B).2 Analyses of the pericardial fluid specific gravity (
Gram's stains in pericardial fluid have a specificity of 99%, but a sensitivity of only 38% for exclusion of the infection in comparison to bacterial cultures.14 Combination of epithelial membrane antigen, CEA and vimentin immunocytochemical staining can be useful to distinguish reactive mesothelial and adenocarcinoma cells.101
Introduction of pericardioscopy and contemporary pathology, virology, and molecular biology techniques have improved the diagnostic value of epicardial/pericardial biopsy.2,8,15,16,102–108 Pericardioscopy makes possible to inspect pericardial surface, select the biopsy site, and take numerous samples safely.16 Targeted pericardial/epicardial biopsy during pericardioscopy was particularly useful in the diagnosis of neoplastic pericarditis.15,16,102–104 No major complications occurred in any of the flexible pericardioscopy studies. Mortality reported in the studies with rigid endoscopes was 2.1%,15 and 3.5%103 due to induction of anaesthesia in patients with very large pericardial effusions.
Histology of epicardial/pericardial biopsies can establish the diagnosis in patients with neoplastic pericarditis and tuberculosis.16,63,102,103 Diagnosis of viral pericarditis can be established by PCR techniques with much higher sensitivity and specificity in comparison to viral isolation from fluid and tissue.107–111 Immunohistochemistry, especially IgG-, IgM- and IgA- and complement fixation contribute significantly to the diagnostic value of epicardial biopsy.2 Specificity of immunoglobulin fixation in autoreactive pericarditis is 100%. Complement fixation was found primarily in patients with the autoreactive form and rarely in patients with neoplastic pericarditis.8 Malignant mesotheliomas can be distinguished from pulmonary adenocarcinomas by immunohistochemical staining for CEA, surfactant apoprotein, Lewis a, and Tn antigen.112
Corresponding author. Chairperson: Bernhard Maisch, MD, FESC, FACC, Dean of the Faculty of Medicine, Director of the Department of Internal Medicine-Cardiology, Philipps University, Marburg, Baldingerstrasse 1, D-35033 Marburg, Germany. Tel.: +49-6421-286-6462; fax: +49-6421-286-8954, E-mail address: bermaisch@aol.com
Members of the Task Force have the pleasure to acknowledge participation of Prof. Dr. Annalisa Angelini (Padua, I) and Dr. Steffen Lamparter (Marburg, D) in preparation of the sections of the Statement on pericardial pathology and analyses of pericardial effusion as well as the kind technical assistance of Ms. Veronica Dean (European Heart House). Special thanks to Professor Eloïsa Arbustini (Pavia, I) for her significant contribution to the review process of these guidelines.
References
Seferović PM, Ristić AD, Maksimović R et al. Therapeutic pericardiocentesis: up-to-date review of indications, efficacy, and risks. In: Seferović PM, Spodick DH, Maisch B, editors, Maksimović R, Ristić AD, assoc. editors. Pericardiology: contemporary answers to continuing challenges, Belgrade, Science 2000;417–26.
Shabetai R. Pulsus paradoxus: definition, mechanisms, and clinical association. In: Seferović PM, Spodick DH, Maisch B, editors., Maksimović R, Ristić AD, assoc. editors. Pericardiology: contemporary answers to continuing challenges, Belgrade, Science 2000;53–62.
Simeunović D, Seferović PM, Ristić AD et al. Pericardial cysts: Incidence, clinical presentations and treatment. In: Seferović PM, Spodick DH, Maisch B, editors. Maksimović R, Ristić AD, assoc. editors. Pericardiology: contemporary answers to continuing challenges, Belgrade, Science 2000;203–12.
Ristić AD, Seferović PM, Maksimović R et al. Percutaneous balloon pericardiotomy in neoplastic pericardial effusion. In: Seferović PM, Spodick DH, Maisch B, editors. Maksimović R, Ristić AD, assoc. editors. Pericardiology: contemporary answers to continuing challenges, Belgrade; Science 2000;427–38.


{kind=link}
{kind=link}