





Abstract
Hysterectomy for benign indications is one of the commonest surgical procedures in women, but the association between the procedure and cardiovascular disease (CVD) is not fully understood. In this population-based cohort study, we studied the effects of hysterectomy, with or without oopherectomy, on the risk of later life CVD.
Using nationwide healthcare registers, we identified all Swedish women having a hysterectomy on benign indications between 1973 and 2003 (n = 184 441), and non-hysterectomized controls (n = 640 043). Main outcome measure was the first hospitalization or death of incident CVD (coronary heart disease, stroke, or heart failure). Occurrence of CVD was determined by individual linkage to the Inpatient Register. In women below age 50 at study entry, hysterectomy was associated with a significantly increased risk of CVD during follow-up [hazard ratio (HR), 1.18, 95% confidence interval (CI), 1.13–1.23; HR, 2.22, 95% CI, 1.01–4.83; and HR, 1.25, 95% CI, 1.06–1.48; in women without oopherectomy, with oopherectomy before or at study entry, respectively, using women without hysterectomy or oopherectomy as reference]. In women aged 50 or above at study entry, there were no significant associations between hysterectomy and incident CVD.
Hysterectomy in women aged 50 years or younger substantially increases the risk for CVD later in life and oopherectomy further adds to the risk of both coronary heart disease and stroke.
Introduction
Hysterectomy has traditionally been considered the method of choice for treating a variety of benign gynaecological disorders due to the low perioperative morbidity and definite cure of these diseases.1 Incidence rates of hysterectomy in the USA and in western European countries have remained relatively stable,2–6 despite recent years introduction of minimally invasive treatment options for conditions, such as menorrhagia and leiomyoma.7
Studies have shown that hysterectomy might be associated with an increased risk for cardiovascular disease (CVD),8–11 but the epidemiological evidence is inconclusive. Previous studies have typically been too small to study associations of hysterectomy with separate types of CVD, such as coronary heart disease and stroke, with adequate statistical strength. Furthermore, temporal relations, such as time elapsed from hysterectomy and oopherectomy (concomitant with the hysterectomy or at a later time point), have been indicated to be of importance for CVD risks but are poorly understood.10
Bilateral salpingo-oopherectomy is the only unambiguous preventive measure for ovarian cancer and results in an abrupt transition to menopause in premenopausal patients. Considering that the majority of hysterectomies is performed in perimenopausal women on relative indications,5,6 increased knowledge about the long-term effects of hysterectomy and/or oopherectomy is critical. Even a moderate risk increase in future disease would be important, as the attributed risk still could be large since hysterectomy is such a common surgical procedure. This is particularly important in the case of CVD, the major cause of death in women globally.12 The aim of this nationwide, population-based cohort study using prospectively recorded data from the Swedish national health registers was to assess the risk of CVD after hysterectomy for benign indications, with or without oopherectomy, throughout the lifespan.
Methods
Ascertainment of data
The Swedish Inpatient Register contains data on individual hospital discharges and contains (i) the dates of hospital admission and discharge; (ii) up to eight discharge diagnoses, coded according to the International Classification of Diseases (ICD) versions 7–10; and (iii) up to 12 operation codes from the Swedish Classification of Operations and Major Procedures. Correct coding for surgical procedures is achieved in 98% of the records.13 The Inpatient Register also includes information about the unique national registration number (NRN), assigned to all Swedish residents, allowing unambiguous record linkage across all nationwide registers in Sweden.
The Cause of Death Register includes information about date and cause of death on all Swedish residents with a completeness exceeding 99%. The Register of Population and Population Changes includes information about dates of birth, death, emigration, and immigration of all Swedish residents. Information on socioeconomic status was retrieved from the Census 1990.
Study population
We identified all records in the Inpatient Register indicating hysterectomy (study entry) from 1 January 1973, through 31 December 2003. To each patient with hysterectomy (n = 227 389), we randomly selected a control (n = 682 167) from the Register of the Total Population, who were individually matched by year of birth and county of residence at the year of hysterectomy. Using NRNs, our exposed and unexposed cohorts (i.e. women with and without hysterectomy) were linked to the Birth Register, Cancer Register, Emigration Register, and Cause of Death Register.
Within the Inpatient Register, we identified all women in the exposed and unexposed cohorts with a recorded CVD. In order to avoid bias introduced by CVD events occurring in relation to the surgical procedure, hysterectomized women contributed person-time to the study from 30 days after hysterectomy until first occurrence of a CVD, heart failure, cervical, corpus or ovarian cancer, death, emigration, or the end of the observation period (31 December 2003). Control women contributed person-time by the same criteria, but with start of follow-up 30 days after the date of matching, i.e. date of hysterectomy of the corresponding hysterectomized woman. We excluded from the analysis women: with incorrect information in the registers (n = 963); with CVD before entry (n = 17 889), with heart failure before start of follow-up (n = 2119), with hysterectomy on malignant indications or cervical, corpus or ovarian cancer registered within 365 days prior to hysterectomy/matching date (n = 37 642); with hysterectomy at age less than 18 years (n = 140); who died at/before start of follow-up (n = 165); who emigrated at/before start of follow-up (n = 12); or with start of follow-up after the end of the observation period (n = 2260). Women with the same values for matching variables were aggregated in order to achieve higher power, by combining the 1:3 matching strata into n:m matching strata. Thereafter, n:m strata containing either only hysterectomized or only non-hysterectomized women were excluded (n = 14 878), because they were deemed non-informative in the analysis. Thus, our final eligible study sample included 184 441 women with hysterectomy and 649 043 individually matched controls.
Classification of exposures and outcomes
The Swedish Classification of Operations and Major Procedures for 1973–1996 and 1997–2003 were used to identify: (i) hysterectomy in the Swedish Inpatient Register (operation codes 7210, 7211, 7261, 7262, 7467 for 1973–1996, and LCD00, LCC10, LCD10, LCD11, LCD01-LCD04, LEF13 for 1997–2003) categorized as yes or no; and 2) oopherectomy performed concurrent with the hysterectomy or by itself, either bilateral once or unilateral twice (operation codes 7020, 7021, 7030, 7031, 7032, LAE10, LAE11, LAE20, LAE21, LAF00, LAF01, LAF10, LAF11, LAF20).
Incidence of CVD was defined as the first hospitalization (assessed from the Hospital Discharge Register) or death (assessed from the Cause of Death Register) caused by coronary heart disease, stroke, or heart failure. Coronary heart disease was defined as unstable angina (ICD-8 code 411, ICD-9 code 411B, ICD-10 code I20.0) or acute myocardial infarction (ICD-8 and ICD-9 code 410, ICD-10 codes I21–I22). Stroke was defined as cerebral infarction (ICD-8 codes 432–434, ICD-9 codes 433–434, ICD-10 code I63), cerebral haemorrhage (ICD-8 code 431, ICD-9 codes 431–432, ICD-10 codes I61–I62), subarachnoidal haemorrhage (ICD-8 and ICD-9 code 430, ICD-10 code I60), transient ischaemic attack (ICD-8 and ICD-9 code 435, ICD-10 code G45), or other acute stroke (ICD-8 and ICD-9 code 436, ICD-10 code I64). Heart failure was defined by ICD-8 codes 427.00 and 427.10, ICD-9 code 428, ICD-10 code I50. We only considered hospitalizations or deaths with the above diagnoses as primary diagnosis of the hospitalization or the primary cause of death. The validity of the stroke,14 myocardial infarction,14,15 and heart failure,16 diagnoses in the Swedish hospital discharge register have been demonstrated to be ∼95% when primary diagnoses are considered.
Statistical analysis
We calculated crude incidence rates for CVD as the number of CVD events per 1000 person-years, with 95% confidence intervals (CIs) based on the Poisson distribution. Only the first occurrence of CVD in each individual was counted as an event. Rates were calculated separately by age (categorized as 18–49 years or ≥50 years), by hysterectomy (categorized as yes or no) and oopherectomy (categorized as never; before hysterectomy; at hysterectomy; or after hysterectomy). Categorization of age as 18–49 years or ≥50 years was based on 50 years being the median age of onset of menopause in Sweden.17 Person time at risk was calculated from 30 days after the date of hysterectomy (exposed cohort) or from the date of matching (unexposed cohort), until the first occurrence of CVD or censoring.
Because we did not have access to information on smoking from the registers we investigated whether women with a hysterectomy were at increased risk for lung cancer as a proxy measure of smoking exposure. If women having hysterectomy are more inclined to smoke they would not only be at increased risk for CVD, but also for lung cancer, compared with women not having a hysterectomy.
Measures of association between exposures and subsequent CVD were investigated using conditional Cox proportional hazards models to retain and take the subject-level matching into account in the analysis. Data were presented as hazard ratios (HRs) with 95% CIs. Women with the same combination of matching variables (age, county, and calendar time) were collapsed into the same strata to gain statistical efficiency. We present HRs separately categorized by age, as well as, hysterectomy, and oopherectomy status (reference group ‘no hysterectomy, never oopherectomy’). We performed two multivariate models: first, adjusting for time since start of follow-up, age, year, and county (model A) and second, further adjusting for socioeconomic status (data available for 71% of the cohort) as a covariate (model B). Oopherectomy was treated as a time-varying covariate in these analyses, i.e. a woman was considered as exposed to oopherectomy only from the time of operation. We used likelihood ratio tests (two-sided, 5% significance level) to assess the effect of exposure. Statistical analyses were performed using Intercooled Stata™ release 9 (StataCorp LP, College Station, TX, USA).
The study was approved by the regional ethical review board at Karolinska Institutet, Stockholm, Sweden and reporting conform to the STROBE guidelines for observational studies (http://www.strobe-statement.org).
Results
During the observation period of our study, 184 441 women having a hysterectomy fulfilled the inclusion criteria (exposed cohort) and were individually matched to 649 043 women not undergoing hysterectomy (unexposed cohort). The median follow-up time was 10.4 years (range 0–31.6; 25–75th percentile, 5.0–17.1) contributing to 9 635 123 person-years at risk and a total of 51 181 CVD events.
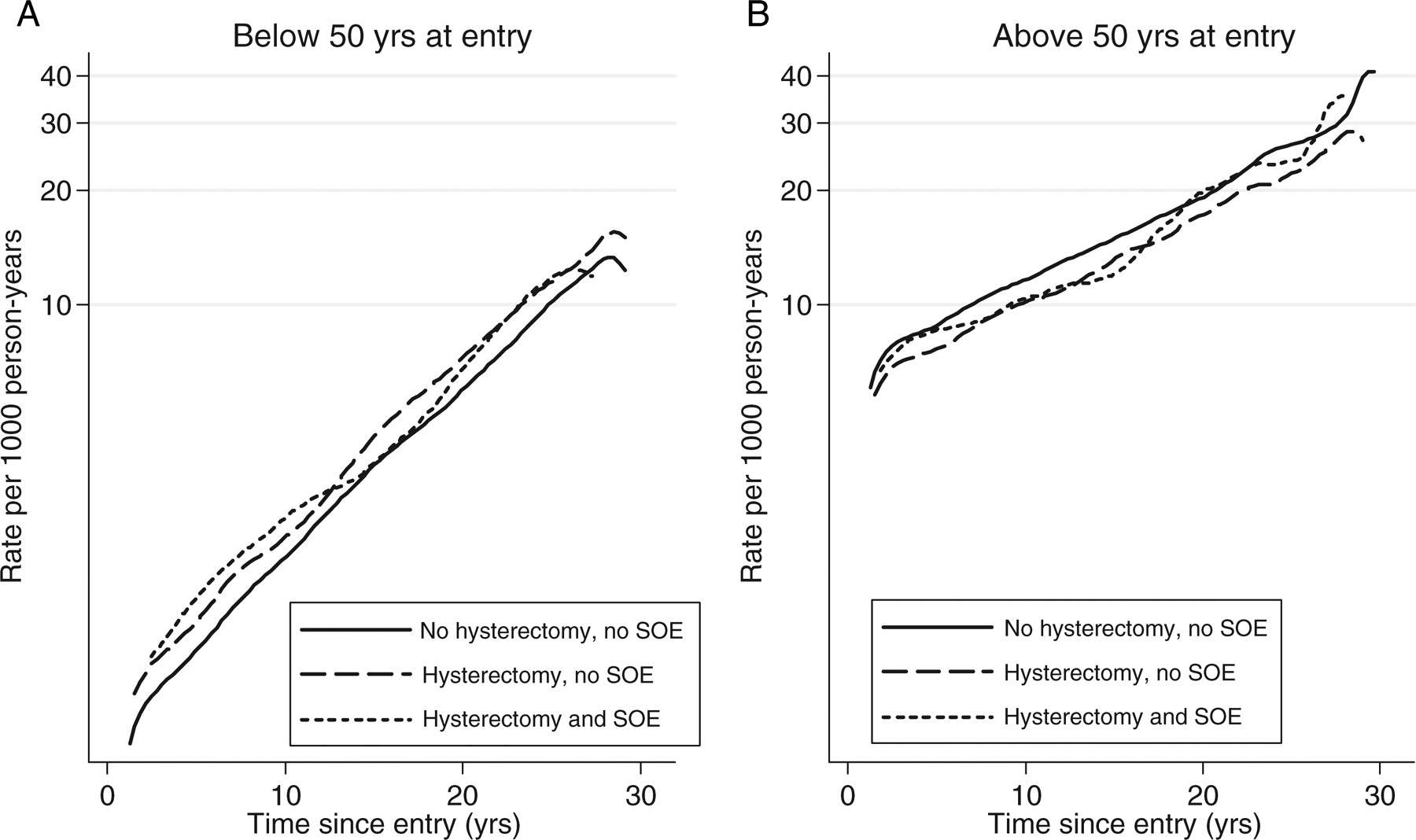
To be able to separate effects of hysterectomy from those of oopherectomy, we took the occurrence and timing of oopherectomy (when present) into account in our analyses. During the observation period, 28 136 of the hysterectomized and 5118 of the non-hysterectomized women had an oopherectomy before, at or after entry in the study (i.e. date of hysterectomy or matching). Table 1 shows the distribution of women with or without hysterectomy and oopherectomy, respectively, along with person-years, number of CVD events and rates (composite or separately for coronary heart disease and stroke) by hysterectomy/oopherectomy category. As expected, the CVD rates were generally higher in the stratum of women over age 50 at entry than in the younger age group. Among younger women, the CVD incidence rates were higher in those that underwent surgical procedures, whereas a reverse pattern was observed in women over age 50 at study entry (Figure 1 and Table 1). There was no excess risk of lung cancer among women with hysterectomy compared with those without (HR 1.0, 95% CI 1.0–1.1) suggesting that the association between hysterectomy and CVD was not confounded by smoking.
Study sample characteristics with rates of cardiovascular diseases by age group and mode of surgery
| Age (years) | Hysterectomy | Oopherectomy | n | Person-years | No. of CVD events | CVDa rateb (95% CI) | No. of CHD events (rateb) | No. of stroke events (rateb) |
|---|---|---|---|---|---|---|---|---|
| ≤49 | No | No | 359 363 | 4 776 655 | 12 003 | 2.5 (2.5–2.6) | 5440 (1.1) | 6565 (1.4) |
| No | Before/at entry | 358 | 4326 | 10 | 2.3 (1.2–4.3) | 5 (1.2) | 5 (1.2) | |
| No | After entry | 1760 | 31 556 | 97 | 3.1 (2.5–3.7) | 46 (1.5) | 51 (1.6) | |
| Yes | No | 104 770 | 1 391 680 | 4103 | 2.9 (2.9–3.0) | 1828 (1.3) | 2275 (1.6) | |
| Yes | Before entry | 181 | 1889 | 7 | 3.7 (1.8–7.8) | 3 (1.6) | 4 (2.1) | |
| Yes | At entry | 5933 | 63 092 | 230 | 3.6 (3.2–4.1) | 103 (1.6) | 127 (2.0) | |
| Yes | After entry | 2233 | 33 782 | 71 | 2.1 (1.7–2.7) | 28 (0.8) | 43 (1.3) | |
| 50≤ | No | No | 284 562 | 2 662 551 | 28 314 | 10.6 (10.5–10.8) | 12 006 (4.5) | 16 313 (6.1) |
| No | Before/at entry | 1721 | 12 821 | 150 | 11.7 (10.0–13.7) | 59 (4.6) | 91 (7.1) | |
| No | After entry | 1279 | 18 047 | 110 | 6.1 (5.1–7.3) | 43 (2.4) | 67 (3.7) | |
| Yes | No | 51 535 | 506 066 | 4768 | 9.4 (9.2–9.7) | 1946 (3.8) | 2823 (5.6) | |
| Yes | Before entry | 481 | 2935 | 33 | 11.2 (8.0–15.8) | 12 (4.1) | 21 (4.7) | |
| Yes | At entry | 18 977 | 126 135 | 1262 | 10.0 (9.5–10.6) | 507 (4.0) | 755 (6.0) | |
| Yes | After entry | 331 | 3588 | 23 | 6.4 (4.3–9.6) | 8 (2.2) | 15 (4.2) |
| Age (years) | Hysterectomy | Oopherectomy | n | Person-years | No. of CVD events | CVDa rateb (95% CI) | No. of CHD events (rateb) | No. of stroke events (rateb) |
|---|---|---|---|---|---|---|---|---|
| ≤49 | No | No | 359 363 | 4 776 655 | 12 003 | 2.5 (2.5–2.6) | 5440 (1.1) | 6565 (1.4) |
| No | Before/at entry | 358 | 4326 | 10 | 2.3 (1.2–4.3) | 5 (1.2) | 5 (1.2) | |
| No | After entry | 1760 | 31 556 | 97 | 3.1 (2.5–3.7) | 46 (1.5) | 51 (1.6) | |
| Yes | No | 104 770 | 1 391 680 | 4103 | 2.9 (2.9–3.0) | 1828 (1.3) | 2275 (1.6) | |
| Yes | Before entry | 181 | 1889 | 7 | 3.7 (1.8–7.8) | 3 (1.6) | 4 (2.1) | |
| Yes | At entry | 5933 | 63 092 | 230 | 3.6 (3.2–4.1) | 103 (1.6) | 127 (2.0) | |
| Yes | After entry | 2233 | 33 782 | 71 | 2.1 (1.7–2.7) | 28 (0.8) | 43 (1.3) | |
| 50≤ | No | No | 284 562 | 2 662 551 | 28 314 | 10.6 (10.5–10.8) | 12 006 (4.5) | 16 313 (6.1) |
| No | Before/at entry | 1721 | 12 821 | 150 | 11.7 (10.0–13.7) | 59 (4.6) | 91 (7.1) | |
| No | After entry | 1279 | 18 047 | 110 | 6.1 (5.1–7.3) | 43 (2.4) | 67 (3.7) | |
| Yes | No | 51 535 | 506 066 | 4768 | 9.4 (9.2–9.7) | 1946 (3.8) | 2823 (5.6) | |
| Yes | Before entry | 481 | 2935 | 33 | 11.2 (8.0–15.8) | 12 (4.1) | 21 (4.7) | |
| Yes | At entry | 18 977 | 126 135 | 1262 | 10.0 (9.5–10.6) | 507 (4.0) | 755 (6.0) | |
| Yes | After entry | 331 | 3588 | 23 | 6.4 (4.3–9.6) | 8 (2.2) | 15 (4.2) |
aCardiovascular disease was defined as the composite of coronary heart disease and stroke.
bRate per 1000 person-years stratified on the matching variables: age, calendar time, and county.
Study sample characteristics with rates of cardiovascular diseases by age group and mode of surgery
| Age (years) | Hysterectomy | Oopherectomy | n | Person-years | No. of CVD events | CVDa rateb (95% CI) | No. of CHD events (rateb) | No. of stroke events (rateb) |
|---|---|---|---|---|---|---|---|---|
| ≤49 | No | No | 359 363 | 4 776 655 | 12 003 | 2.5 (2.5–2.6) | 5440 (1.1) | 6565 (1.4) |
| No | Before/at entry | 358 | 4326 | 10 | 2.3 (1.2–4.3) | 5 (1.2) | 5 (1.2) | |
| No | After entry | 1760 | 31 556 | 97 | 3.1 (2.5–3.7) | 46 (1.5) | 51 (1.6) | |
| Yes | No | 104 770 | 1 391 680 | 4103 | 2.9 (2.9–3.0) | 1828 (1.3) | 2275 (1.6) | |
| Yes | Before entry | 181 | 1889 | 7 | 3.7 (1.8–7.8) | 3 (1.6) | 4 (2.1) | |
| Yes | At entry | 5933 | 63 092 | 230 | 3.6 (3.2–4.1) | 103 (1.6) | 127 (2.0) | |
| Yes | After entry | 2233 | 33 782 | 71 | 2.1 (1.7–2.7) | 28 (0.8) | 43 (1.3) | |
| 50≤ | No | No | 284 562 | 2 662 551 | 28 314 | 10.6 (10.5–10.8) | 12 006 (4.5) | 16 313 (6.1) |
| No | Before/at entry | 1721 | 12 821 | 150 | 11.7 (10.0–13.7) | 59 (4.6) | 91 (7.1) | |
| No | After entry | 1279 | 18 047 | 110 | 6.1 (5.1–7.3) | 43 (2.4) | 67 (3.7) | |
| Yes | No | 51 535 | 506 066 | 4768 | 9.4 (9.2–9.7) | 1946 (3.8) | 2823 (5.6) | |
| Yes | Before entry | 481 | 2935 | 33 | 11.2 (8.0–15.8) | 12 (4.1) | 21 (4.7) | |
| Yes | At entry | 18 977 | 126 135 | 1262 | 10.0 (9.5–10.6) | 507 (4.0) | 755 (6.0) | |
| Yes | After entry | 331 | 3588 | 23 | 6.4 (4.3–9.6) | 8 (2.2) | 15 (4.2) |
| Age (years) | Hysterectomy | Oopherectomy | n | Person-years | No. of CVD events | CVDa rateb (95% CI) | No. of CHD events (rateb) | No. of stroke events (rateb) |
|---|---|---|---|---|---|---|---|---|
| ≤49 | No | No | 359 363 | 4 776 655 | 12 003 | 2.5 (2.5–2.6) | 5440 (1.1) | 6565 (1.4) |
| No | Before/at entry | 358 | 4326 | 10 | 2.3 (1.2–4.3) | 5 (1.2) | 5 (1.2) | |
| No | After entry | 1760 | 31 556 | 97 | 3.1 (2.5–3.7) | 46 (1.5) | 51 (1.6) | |
| Yes | No | 104 770 | 1 391 680 | 4103 | 2.9 (2.9–3.0) | 1828 (1.3) | 2275 (1.6) | |
| Yes | Before entry | 181 | 1889 | 7 | 3.7 (1.8–7.8) | 3 (1.6) | 4 (2.1) | |
| Yes | At entry | 5933 | 63 092 | 230 | 3.6 (3.2–4.1) | 103 (1.6) | 127 (2.0) | |
| Yes | After entry | 2233 | 33 782 | 71 | 2.1 (1.7–2.7) | 28 (0.8) | 43 (1.3) | |
| 50≤ | No | No | 284 562 | 2 662 551 | 28 314 | 10.6 (10.5–10.8) | 12 006 (4.5) | 16 313 (6.1) |
| No | Before/at entry | 1721 | 12 821 | 150 | 11.7 (10.0–13.7) | 59 (4.6) | 91 (7.1) | |
| No | After entry | 1279 | 18 047 | 110 | 6.1 (5.1–7.3) | 43 (2.4) | 67 (3.7) | |
| Yes | No | 51 535 | 506 066 | 4768 | 9.4 (9.2–9.7) | 1946 (3.8) | 2823 (5.6) | |
| Yes | Before entry | 481 | 2935 | 33 | 11.2 (8.0–15.8) | 12 (4.1) | 21 (4.7) | |
| Yes | At entry | 18 977 | 126 135 | 1262 | 10.0 (9.5–10.6) | 507 (4.0) | 755 (6.0) | |
| Yes | After entry | 331 | 3588 | 23 | 6.4 (4.3–9.6) | 8 (2.2) | 15 (4.2) |
aCardiovascular disease was defined as the composite of coronary heart disease and stroke.
bRate per 1000 person-years stratified on the matching variables: age, calendar time, and county.
Incidence rates over time of cardiovascular disease (composite of coronary heart disease and stroke) in women below or above age 50 at baseline by mode of surgical procedure.
In women below age 50 at study entry, hysterectomy was associated with a significantly higher risk of CVD during follow-up (Table 2, upper panel). In models taking age, calendar time, county, and socioeconomic status into account, this risk increase was ∼20% in women that did not go through an oopherectomy at all, or had an oopherectomy at the same time as the hysterectomy. In women who had an oopherectomy before study entry, and then a hysterectomy, the point estimate was higher, but this analysis was based on very few CVD events (n = 7); hence, the CI was very wide and the result borderline significant.
Associations of hysterectomy and/or oophorectomy with cardiovascular disease by age group and mode of surgerya
| Age (years) | Hysterectomy | Oopherectomy | HR (95% CI) | |||
|---|---|---|---|---|---|---|
| Model Ab | Model Bc | |||||
| ≤49 | No | No | 1.0 | Reference | 1.0 | Reference |
| No | Before/at entry | 0.80 | (0.43–1.49) | 0.98 | (0.48–1.97) | |
| No | After entry | 0.98 | (0.80–1.19) | 1.08 | (0.84–1.37) | |
| Yes | No | 1.18 | (1.14–1.22) | 1.18 | (1.13–1.23) | |
| Yes | Before entry | 1.69 | (0.79–3.64) | 2.22 | (1.01–4.83) | |
| Yes | At entry | 1.10 | (0.97–1.26) | 1.25 | (1.06–1.48) | |
| Yes | After entry | 0.91 | (0.72–1.15) | 1.03 | (0.79–1.33) | |
| 50≤ | No | No | 1.0 | Reference | 1.0 | Reference |
| No | Before/at entry | 0.97 | (0.82–1.15) | 0.99 | (0.69–1.41) | |
| No | After entry | 0.59 | (0.48–0.71) | 0.56 | (0.35–0.90) | |
| Yes | No | 0.97 | (0.94–1.00) | 0.94 | (0.88–1.00) | |
| Yes | Before entry | 1.01 | (0.71–1.45) | 0.61 | (0.27–1.41) | |
| Yes | At entry | 1.02 | (0.96–1.09) | 0.95 | (0.85–1.08) | |
| Yes | After entry | 0.83 | (0.54–1.26) | 0.89 | (0.43–1.81) | |
| Age (years) | Hysterectomy | Oopherectomy | HR (95% CI) | |||
|---|---|---|---|---|---|---|
| Model Ab | Model Bc | |||||
| ≤49 | No | No | 1.0 | Reference | 1.0 | Reference |
| No | Before/at entry | 0.80 | (0.43–1.49) | 0.98 | (0.48–1.97) | |
| No | After entry | 0.98 | (0.80–1.19) | 1.08 | (0.84–1.37) | |
| Yes | No | 1.18 | (1.14–1.22) | 1.18 | (1.13–1.23) | |
| Yes | Before entry | 1.69 | (0.79–3.64) | 2.22 | (1.01–4.83) | |
| Yes | At entry | 1.10 | (0.97–1.26) | 1.25 | (1.06–1.48) | |
| Yes | After entry | 0.91 | (0.72–1.15) | 1.03 | (0.79–1.33) | |
| 50≤ | No | No | 1.0 | Reference | 1.0 | Reference |
| No | Before/at entry | 0.97 | (0.82–1.15) | 0.99 | (0.69–1.41) | |
| No | After entry | 0.59 | (0.48–0.71) | 0.56 | (0.35–0.90) | |
| Yes | No | 0.97 | (0.94–1.00) | 0.94 | (0.88–1.00) | |
| Yes | Before entry | 1.01 | (0.71–1.45) | 0.61 | (0.27–1.41) | |
| Yes | At entry | 1.02 | (0.96–1.09) | 0.95 | (0.85–1.08) | |
| Yes | After entry | 0.83 | (0.54–1.26) | 0.89 | (0.43–1.81) | |
aValues are Cox regression hazard ratios and 95% confidence intervals (95% CI) for cardiovascular disease incidence, with time of follow-up as timescale.
bAnalysis stratified on the matching variables: age, calendar time, and county.
cAnalyses additionally adjusted for socioeconomic status.
Associations of hysterectomy and/or oophorectomy with cardiovascular disease by age group and mode of surgerya
| Age (years) | Hysterectomy | Oopherectomy | HR (95% CI) | |||
|---|---|---|---|---|---|---|
| Model Ab | Model Bc | |||||
| ≤49 | No | No | 1.0 | Reference | 1.0 | Reference |
| No | Before/at entry | 0.80 | (0.43–1.49) | 0.98 | (0.48–1.97) | |
| No | After entry | 0.98 | (0.80–1.19) | 1.08 | (0.84–1.37) | |
| Yes | No | 1.18 | (1.14–1.22) | 1.18 | (1.13–1.23) | |
| Yes | Before entry | 1.69 | (0.79–3.64) | 2.22 | (1.01–4.83) | |
| Yes | At entry | 1.10 | (0.97–1.26) | 1.25 | (1.06–1.48) | |
| Yes | After entry | 0.91 | (0.72–1.15) | 1.03 | (0.79–1.33) | |
| 50≤ | No | No | 1.0 | Reference | 1.0 | Reference |
| No | Before/at entry | 0.97 | (0.82–1.15) | 0.99 | (0.69–1.41) | |
| No | After entry | 0.59 | (0.48–0.71) | 0.56 | (0.35–0.90) | |
| Yes | No | 0.97 | (0.94–1.00) | 0.94 | (0.88–1.00) | |
| Yes | Before entry | 1.01 | (0.71–1.45) | 0.61 | (0.27–1.41) | |
| Yes | At entry | 1.02 | (0.96–1.09) | 0.95 | (0.85–1.08) | |
| Yes | After entry | 0.83 | (0.54–1.26) | 0.89 | (0.43–1.81) | |
| Age (years) | Hysterectomy | Oopherectomy | HR (95% CI) | |||
|---|---|---|---|---|---|---|
| Model Ab | Model Bc | |||||
| ≤49 | No | No | 1.0 | Reference | 1.0 | Reference |
| No | Before/at entry | 0.80 | (0.43–1.49) | 0.98 | (0.48–1.97) | |
| No | After entry | 0.98 | (0.80–1.19) | 1.08 | (0.84–1.37) | |
| Yes | No | 1.18 | (1.14–1.22) | 1.18 | (1.13–1.23) | |
| Yes | Before entry | 1.69 | (0.79–3.64) | 2.22 | (1.01–4.83) | |
| Yes | At entry | 1.10 | (0.97–1.26) | 1.25 | (1.06–1.48) | |
| Yes | After entry | 0.91 | (0.72–1.15) | 1.03 | (0.79–1.33) | |
| 50≤ | No | No | 1.0 | Reference | 1.0 | Reference |
| No | Before/at entry | 0.97 | (0.82–1.15) | 0.99 | (0.69–1.41) | |
| No | After entry | 0.59 | (0.48–0.71) | 0.56 | (0.35–0.90) | |
| Yes | No | 0.97 | (0.94–1.00) | 0.94 | (0.88–1.00) | |
| Yes | Before entry | 1.01 | (0.71–1.45) | 0.61 | (0.27–1.41) | |
| Yes | At entry | 1.02 | (0.96–1.09) | 0.95 | (0.85–1.08) | |
| Yes | After entry | 0.83 | (0.54–1.26) | 0.89 | (0.43–1.81) | |
aValues are Cox regression hazard ratios and 95% confidence intervals (95% CI) for cardiovascular disease incidence, with time of follow-up as timescale.
bAnalysis stratified on the matching variables: age, calendar time, and county.
cAnalyses additionally adjusted for socioeconomic status.
In women aged 50 or above at study entry, having a hysterectomy was associated with a slightly lower risk of CVD during follow-up. This risk decrease was borderline significant in women without oopherectomy, but non-significant in women with oopherectomy in addition to their hysterectomy (before, at or after study entry; Table 2, lower panel). Further, in this older age group, among women that did not have a hysterectomy, but that went through an oopherectomy after study entry, there was a >40% lower risk of CVD during follow-up.
Using models with oopherectomy as a time-varying covariate, the same patterns with differences across the two age categories emerged (Table 3). In women under age 50 at study entry, both hysterectomy and oopherectomy were independently associated with an increased risk of CVD during follow-up. This risk increase was rather substantial; almost 20% and >40% higher CVD risk, respectively. Further, the risk increase was consistent for incidence in coronary heart disease and stroke. In women aged 50 or above at study entry, hysterectomy was borderline significantly associated with a lower risk of CVD and coronary heart disease during follow-up, whereas there were no association of oopherectomy and CVD in this age category.
Associations of hysterectomy and/or oophorectomy with different types of cardiovascular disease in models with oophorectomy as a time-varying covariatea
| Age (years) | Hysterectomy | HR (95% CI) | |||
|---|---|---|---|---|---|
| Models Ab | Models Bc | ||||
| CVDd | |||||
| 18–49 | Hysterectomy | 1.17 | (1.13–1.21) | 1.17 | (1.13–1.22) |
| Oophorectomy | 1.31 | (1.12–1.53) | 1.44 | (1.20–1.73) | |
| 50≤ | Hysterectomy | 0.97 | (0.94–1.00) | 0.94 | (0.88–1.00) |
| Oophorectomy | 0.98 | (0.82–1.18) | 0.92 | (0.61–1.38) | |
| CHD | |||||
| 18–49 | Hysterectomy | 1.15 | (1.09–1.21) | 1.16 | (1.09–1.24) |
| Oophorectomy | 1.30 | (1.03–1.64) | 1.40 | (1.06–1.84) | |
| 50≤ | Hysterectomy | 0.94 | (0.89–0.98) | 0.90 | (0.81–0.99) |
| Oophorectomy | 0.88 | (0.65–1.18) | 0.83 | (0.45–1.55) | |
| Stroke | |||||
| 18–49 | Hysterectomy | 1.19 | (1.13–1.25) | 1.18 | (1.12–1.25) |
| Oophorectomy | 1.33 | (1.08–1.64) | 1.47 | (1.16–1.87) | |
| 50≤ | Hysterectomy | 1.00 | (0.96–1.04) | 0.97 | (0.89–1.06) |
| Oophorectomy | 1.06 | (0.84–1.34) | 0.99 | (0.58–1.69) | |
| Age (years) | Hysterectomy | HR (95% CI) | |||
|---|---|---|---|---|---|
| Models Ab | Models Bc | ||||
| CVDd | |||||
| 18–49 | Hysterectomy | 1.17 | (1.13–1.21) | 1.17 | (1.13–1.22) |
| Oophorectomy | 1.31 | (1.12–1.53) | 1.44 | (1.20–1.73) | |
| 50≤ | Hysterectomy | 0.97 | (0.94–1.00) | 0.94 | (0.88–1.00) |
| Oophorectomy | 0.98 | (0.82–1.18) | 0.92 | (0.61–1.38) | |
| CHD | |||||
| 18–49 | Hysterectomy | 1.15 | (1.09–1.21) | 1.16 | (1.09–1.24) |
| Oophorectomy | 1.30 | (1.03–1.64) | 1.40 | (1.06–1.84) | |
| 50≤ | Hysterectomy | 0.94 | (0.89–0.98) | 0.90 | (0.81–0.99) |
| Oophorectomy | 0.88 | (0.65–1.18) | 0.83 | (0.45–1.55) | |
| Stroke | |||||
| 18–49 | Hysterectomy | 1.19 | (1.13–1.25) | 1.18 | (1.12–1.25) |
| Oophorectomy | 1.33 | (1.08–1.64) | 1.47 | (1.16–1.87) | |
| 50≤ | Hysterectomy | 1.00 | (0.96–1.04) | 0.97 | (0.89–1.06) |
| Oophorectomy | 1.06 | (0.84–1.34) | 0.99 | (0.58–1.69) | |
aValues are Cox regression hazard ratios and 95% confidence intervals (95% CI) for cardiovascular disease incidence, with time of follow-up as time scale and oopherectomy as a time-varying covariate.
bAnalysis stratified on the matching variables: age, calendar time and county.
cAnalyses additionally adjusted for socioeconomic status.
dCardiovascular disease was defined as the composite of coronary heart disease and stroke.
Associations of hysterectomy and/or oophorectomy with different types of cardiovascular disease in models with oophorectomy as a time-varying covariatea
| Age (years) | Hysterectomy | HR (95% CI) | |||
|---|---|---|---|---|---|
| Models Ab | Models Bc | ||||
| CVDd | |||||
| 18–49 | Hysterectomy | 1.17 | (1.13–1.21) | 1.17 | (1.13–1.22) |
| Oophorectomy | 1.31 | (1.12–1.53) | 1.44 | (1.20–1.73) | |
| 50≤ | Hysterectomy | 0.97 | (0.94–1.00) | 0.94 | (0.88–1.00) |
| Oophorectomy | 0.98 | (0.82–1.18) | 0.92 | (0.61–1.38) | |
| CHD | |||||
| 18–49 | Hysterectomy | 1.15 | (1.09–1.21) | 1.16 | (1.09–1.24) |
| Oophorectomy | 1.30 | (1.03–1.64) | 1.40 | (1.06–1.84) | |
| 50≤ | Hysterectomy | 0.94 | (0.89–0.98) | 0.90 | (0.81–0.99) |
| Oophorectomy | 0.88 | (0.65–1.18) | 0.83 | (0.45–1.55) | |
| Stroke | |||||
| 18–49 | Hysterectomy | 1.19 | (1.13–1.25) | 1.18 | (1.12–1.25) |
| Oophorectomy | 1.33 | (1.08–1.64) | 1.47 | (1.16–1.87) | |
| 50≤ | Hysterectomy | 1.00 | (0.96–1.04) | 0.97 | (0.89–1.06) |
| Oophorectomy | 1.06 | (0.84–1.34) | 0.99 | (0.58–1.69) | |
| Age (years) | Hysterectomy | HR (95% CI) | |||
|---|---|---|---|---|---|
| Models Ab | Models Bc | ||||
| CVDd | |||||
| 18–49 | Hysterectomy | 1.17 | (1.13–1.21) | 1.17 | (1.13–1.22) |
| Oophorectomy | 1.31 | (1.12–1.53) | 1.44 | (1.20–1.73) | |
| 50≤ | Hysterectomy | 0.97 | (0.94–1.00) | 0.94 | (0.88–1.00) |
| Oophorectomy | 0.98 | (0.82–1.18) | 0.92 | (0.61–1.38) | |
| CHD | |||||
| 18–49 | Hysterectomy | 1.15 | (1.09–1.21) | 1.16 | (1.09–1.24) |
| Oophorectomy | 1.30 | (1.03–1.64) | 1.40 | (1.06–1.84) | |
| 50≤ | Hysterectomy | 0.94 | (0.89–0.98) | 0.90 | (0.81–0.99) |
| Oophorectomy | 0.88 | (0.65–1.18) | 0.83 | (0.45–1.55) | |
| Stroke | |||||
| 18–49 | Hysterectomy | 1.19 | (1.13–1.25) | 1.18 | (1.12–1.25) |
| Oophorectomy | 1.33 | (1.08–1.64) | 1.47 | (1.16–1.87) | |
| 50≤ | Hysterectomy | 1.00 | (0.96–1.04) | 0.97 | (0.89–1.06) |
| Oophorectomy | 1.06 | (0.84–1.34) | 0.99 | (0.58–1.69) | |
aValues are Cox regression hazard ratios and 95% confidence intervals (95% CI) for cardiovascular disease incidence, with time of follow-up as time scale and oopherectomy as a time-varying covariate.
bAnalysis stratified on the matching variables: age, calendar time and county.
cAnalyses additionally adjusted for socioeconomic status.
dCardiovascular disease was defined as the composite of coronary heart disease and stroke.
Discussion
In the present nationwide cohort study encompassing >800 000 women at risk, we report that having a hysterectomy and/or an oopherectomy before age 50 (corresponding to the median age of onset of menopause in Sweden),17 was associated with a substantially increased risk of later life CVD. This risk increase was consistent for incidence in coronary heart disease, as well as stroke, and it was evident also after taking socioeconomic status into account. In contrast, in women above age 50, hysterectomy as well as oopherectomy was associated with lower risk of CVD during follow-up. The most plausible explanation for this observation is a selection bias where women undergoing elective surgery for benign indications at older ages generally are healthier and at a lower risk for future CVD than those that do not undergo surgery.
The association between hysterectomy and CVD has been suggested to rely on three factors: age at surgery; disruption of ovarian circulation at hysterectomy; and the effects of concomitant bilateral oopherectomy.18 Previous studies are largely in agreement that early surgical menopause increases the risk for CVD,10,19,20 but prospective cohort studies are scarce and results are inconclusive with regard to the effects of simple hysterectomy without oopherectomy. In premenopausal women, bilateral oopherectomy results in an abrupt fall in circulating oestrogens and testosterone levels, and the patient enters menopause immediately. To our knowledge, there are no data to support that surgical menopause leads to hypertension, insulin resistance, or type 2 diabetes, whereas it has been shown to increase total cholesterol and LDL levels.21 Hence, long-standing hypercholesterolaemia may be a mechanism linking surgical menopause with atherosclerosis and clinical CVD.
In women under the age of 50 years, hysterectomy by itself was associated with an increased risk of CVD compared with women with an intact uterus. This finding corroborates the notion that hysterectomy interferes with ovarian blood flow and may result in premature ovarian failure and hormone-related effects on the vascular bed. Having an oopherectomy at the time of the hysterectomy, and in particular before, added further to the risk also after adjusting for socioeconomic status. No previous studies have been stratified for the relation of having a bilateral oopherectomy before, concurrent with, or after the hysterectomy. The adverse cardiovascular effects of hysterectomy, and oopherectomy, were only notable in younger women, which give further corroboration to studies suggesting that it may be the surgical menopause itself that is associated with an increased risk for CVD.11 Thus, the underlying biological rationale for an association between hysterectomy and CVD is likely to be found in ovarian failure. For this reason, information on age at surgery and the timeline of events is important to fully understand the relation, yet data on the intricate relation between hysterectomy, oopherectomy, and cardiovascular morbidity in the general population have been lacking.
Our data are in agreement with a meta-analysis suggesting that bilateral oopherectomy before the age of 50 years increases the overall CVD risk.22 Risk estimates of coronary heart disease of a similar magnitude as those found in the present study were observed in the Nurses Health Study.20 However, in contrast to the Nurses Health Study, we also found a significantly increased risk of stroke. The reason for this difference could be attributed to differences in methodology, where the Nurses’ Health Study relies on voluntary participation and self-reported measures of outcomes, which to some extent may involve selection, ascertainment, and classification bias. If the risk for CVD after hysterectomy and/or oopherectomy is attributed to early surgical menopause and precipitated atherosclerosis, it seems biologically plausible that the risk also applies to cerebral vascularization and stroke.
Data from high-quality nationwide healthcare registers, such as the Swedish Hospital Discharge Register, have proved highly accurate for diagnoses of CVD,14–16 and the register has a negligible loss to registration.13 Furthermore, our data are representative for the general population and controls are drawn from the same population as where cases arose. The register also allows for establishing a temporal chain of events given the prospective data collection. Despite the strengths of our study, use of register data is at the same time a weakness compared with other prospective cohorts, since information on life events not requiring hospitalization goes unregistered. Thus, we may have missed milder cases of CVD that only were treated as outpatients. On the other hand, this would be expected to increase the validity of the endpoints, limiting the inclusion of false positive cases. Another inherent limitation of using nationwide registry data is that we lack information about other CVD risk factors than age and socioeconomic status. We recognize that our study cannot adjust for some factors, such as diabetes and obesity, known to influence the risk of CVD. However, these factors would make women less likely to have abdominal surgery due to co-morbidity and underestimate the risk for CVD attributed to hysterectomy and oopherectomy in our study. Further, there was no indication that smoking confounded the observed associations since the risk for lung cancer was the same for women with and without the surgical procedures. The relatively homogenous population of women living in Sweden is expected to increase the internal validity and reliability of the findings but at the same time the ability to generalize our findings to other populations is unknown and the observational study design cannot infer causality.
Hysterectomy rates of ∼5.5 hysterectomies per 1000 female US resident and 2.1 per 1000 in Sweden6 make hysterectomy the second most common abdominal surgical procedure in women after cesarean delivery. The low perioperative morbidity and cost-effectiveness of the procedure make hysterectomy an attractive and definitive treatment option for a number of gynaecological disorders. Current trends in hysterectomy for benign disorders indicate both a broadening of indications, as well as, a shift towards providing younger women of reproductive and perimenopausal age a definitive surgical solution to gynaecological disorders.6 Thus, our findings of an increased risk of CVD in women having a hysterectomy and/or bilateral oopherectomy in premenopausal age may have global and important implications for women's health.
Funding
By grants from the Swedish Research Council (grant no. 2009–2298) and the Swedish Society of Medicine (E.I.); a grant from the Swedish Society of Medicine (D.A.), and funding from the Regional agreement on clinical research between Stockholm County Council and Karolinska Institutet (D.A.).
Conflict of interest: none declared.


{kind=link}
{kind=link}
Comments
Dear editor,
We read the interesting paper "Hysterectomy and risk of cardiovascular disease: a population-based cohort study" in the European Heart Journal by Ingelsson et al [1]. The study concludes that hysterectomy in women aged 50 years or younger substantially increases the risk for cardiovascular disease (CVD) later in life.
However, as known, for a causal inference to be made, one needs more than an association. The association of hysterectomy and CVD might be strongly modified by the association between hypertension, the main risk factor for CVD and early death [2], and fibroids, the most common cause for hysterectomy [3]. Earlier studies showed a higher prevalence of hypertension in women who had undergone hysterectomies for fibroids, compared to those who had undergone hysterectomies for other reasons [4]. Thus, the increased risk of CVD observed among hysterectomised women might well be explained by the underlying association between uterine fibroids and hypertension [4,5].
Although the authors discuss the limitations of using nationwide registry data, including the lack of information about CVD risk factors other than age and socioeconomic status, they do not mention the association of fibroids with hypertension. Hypertension occurs in 44% in premenopausal women in Sweden [6] and is more frequent in women with fibroids. Consequently, the prevalence of hypertension in the study group could have confounded the outcome of an association between hysterectomy and CVD.
Therefore, we conclude that the higher occurrence of hypertension in premenopausal women with fibroids undergoing a hysterectomy, might contribute to the increased risk for CVD associated with hysterectomy. The authors' finding that hysterectomy raises the risk for CVD might thus be spurious, confounded by the greater occurrence of hypertension in this group.
Sincerely,
Y.C.L. Haan, Dpt. of Vascular Medicine AMC Amsterdam, y.c.haan@amc.nl
REFERENCES
1. Ingelsson E, Lundholm C, Johansson AL, Altman D. Hysterectomy and risk of cardiovascular disease: a population-based cohort study. Eur Heart J. 2011 Mar;32(6):745-50.
2. Ezzati M, Hoorn SV, Rodgers A, Lopez AD, Mathers CD, Murray CJ; Comparative Risk Assessment Collaborating Group. Estimates of global and regional potential health gains from reducing multiple major risk factors. Lancet. 2003 Jul 26;362(9380):271-80.
3. Lundholm C, Forsgren C, Johansson AL, Cnattingius S, Altman D. Hysterectomy on benign indications in Sweden 1987-2003: a nationwide trend analysis. Acta Obstet Gynecol Scand. 2009;88(1):52-8.
4. Silver MA, Raghuvir R, Fedirko B, Elser D. Systemic hypertension among women with uterine leiomyomata: potential final common pathways of target end-organ remodeling. J Clin Hypertens (Greenwich). 2005 Nov;7(11):664-8.
5. Settnes A, Andreasen AH, J?rgensen T. Hypertension is associated with an increased risk for hysterectomy: a Danish cohort study. Eur J Obstet Gynecol Reprod Biol. 2005 Oct 1;122(2):218-24.
6. Khatibi A, Agardh CD, Nyberg P, Lidfeldt J, Samsioe G. Blood pressure in middle-aged women: are androgens involved? A population-based study of Swedish women: the Women's Health in the Lund Area study. J Hypertens. 2007 Oct;25(10):2044-50.
Conflict of Interest:
None declared