





Abstract
Tai Chi has been widely practiced as a Chinese martial art that focuses on slow sequential movements, providing a smooth, continuous and low intensity activity. It has been promoted to improve balance and strength and to reduce falls in the elderly, especially those ‘at risk’. The potential benefits in healthy younger age cohorts and for wider aspects of health have received less attention. The present study documented prospective changes in balance and vascular responses for a community sample of middle-aged women. Seventeen relatively sedentary but healthy normotensive women aged 33–55 years were recruited into a three times per week, 12-week Tai Chi exercise programme. A further 17 sedentary subjects matched for age and body size were recruited as a control group. Dynamic balance measured by the Functional Reach Test was significantly improved following Tai Chi, with significant decreases in both mean systolic (9.71 mmHg) and diastolic (7.53 mmHg) blood pressure. The data confirm that Tai Chi exercise can be a good choice of exercise for middle-aged adults, with potential benefits for ageing as well as the aged.
INTRODUCTION
Tai Chi Chuan or Tai Chi is a widely practiced Chinese martial art. It consists of a series of postures combined in slow, smooth, graceful movements and is considered a low intensity exercise that is claimed to develop balance, coordination, and help maintain strength and emotional health (Koh, 1981; Brown et al., 1989; Wolf et al., 1997; Li, J. X. et al., 2001; Wolf et al., 2001; Wu, 2002). Empirical research on Tai Chi has primarily been directed toward potential benefits for the elderly, with the distal goal of reducing falls (Province et al., 1995; Schaller, 1996; Wolfson et al., 1996; Kutner et al., 1997; Yan, 1998). Evidence based initially on cross-sectional studies has employed improved experimental and longitudinal designs and has further supported the beneficial effects of Tai Chi. However, such outcomes may occur only with prolonged training (Wolfson et al., 1996) and most data have been compiled from populations considered ‘at risk’ (primarily of falls) rather than from wider community populations.
Concern over the social and economic consequences of increasing longevity has also led to consideration of the process of aging rather than the product of that process, the elderly (Thornton, 1992). While there is some debate as to whether increasing levels of regular aerobic exercise conveys increased health benefits, there is consensus that inactivity decreases longevity (Leon et al., 1997).
Tai Chi is considered a low intensity exercise that does convey aerobic benefits (Lai et al., 1993; Li, J. X. et al., 2001). However, benefits of exercise for longevity accrue only with maintained, regular activity and such adherence is problematical for many conventional exercises (Dishman, 1988). Adherence is likely to be dependent on perceived physical as well as psychological outcomes, such as self-efficacy, both of which are enhanced by Tai Chi (Williams and Lord, 1995; Li, F. Z. et al., 2001). Thus it may prove to be an activity that may be sustained over the long-term as suggested by anecdotal data (Lan et al., 2002). However, psychological gains from Tai Chi have been demonstrated only in the elderly, and there is a need therefore to establish benefits in younger age cohorts for whom balance is seldom problematical.
In general, there is a paucity of research on the benefits of Tai Chi for the non-elderly population, possibly because of the unwarranted perception that Tai Chi is an exercise appropriate only for the elderly. Similar benefits may not ensue because Tai Chi for them does not provide discernable, ecological, significant outcomes (such as decreased unsteadiness or falls). Currently, only two studies have documented improvements in static and dynamic sway in age cohorts <60 years of age (Jacobson et al., 1997; Shih, 1997).
Health risks in women in old age, including cardiovascular disease, their enhanced risk of falls, osteoporosis and subsequent bone fracture, have been attributed to a failure to maintain exercise earlier in life (Ferrucci et al., 2000; Stalenhoef, et al., 2002; Terrio and Auld, 2002). The present study documents prospective changes in balance and blood pressure in a community cohort of middle-age women who had previously not participated in formal sports, exercise or Tai Chi sessions. In addition, following pilot work, the study was restricted to women because of the failure to recruit male volunteers in the specified age group. This may be because of testing in a locale where there were prolonged occupational demands on males.
METHODS
Participants
Healthy, community-dwelling women of Chinese ethnicity, aged 33–55 years, body weight 55.3 ± 8.2 kg, height 160.7 ± 3.5 cm, were recruited as an opportunistic sample of volunteers for the study following the posting of leaflets in a local and restricted housing area located close to a park (Tsing Yi) in Honk Kong. The medical history of each individual was reviewed to ensure no contraindications to participation and to confirm they were free from, and had no history of, cardiovascular, pulmonary or musculoskeletal disease. No subject had visited their physician in the previous 6-month period, or were currently taking any medication. They had not previously undertaken Tai Chi practice and all were relatively sedentary in that they had not participated in other forms of sport or exercise for health or recreational purposes for at least 2 years. Twenty randomly selected women from these volunteers agreed to participate in a programme of Tai Chi exercise. The control group comprised a similar sample of healthy subjects living in the same district in similar housing, and recruited in the same manner. They were selected to provide a stratified sample with respect to age, body size and activity/exercise profile with the Tai Chi group. No control subject refused to participate in the study and, if they asked, they were told that they could attend Tai Chi practice after the first phase of the study. After receiving information concerning the study, all participants were asked to sign a form confirming such receipt and consenting to participate in the study.
Procedure
The prospective, treatment-control study design involved pre- and post-measurement tests relating to the 12-week period of Tai Chi exercise. The dependent variables, balance and blood pressure, as well as body height and weight were measured in all subjects. The Tai Chi group participated in a 12-week Tai Chi exercise class held 3 days per week early in the morning in a park in Tsing Yi, Hong Kong. Each exercise session lasted ∼60 min and was led by a certified Tai Chi instructor from the Hong Kong Tai Chi Association. It included 20 min of warm up exercises (including stretching and balancing exercise), 30 min of Tai Chi practice, and was followed by 10 min of cool down exercise (similar to the warm up exercise). The form of Tai Chi, the Yang style, is the most popular form and consists of 108 forms of posture. Subjects imitated the instructor's motions and postures at the same speed. During sessions, the instructor constantly monitored the subjects and corrected the body position, joint angles and form-to-form transition. Compliance with the Tai Chi sessions was documented by session attendance. During the same 12-week period, subjects in the control group were instructed to continue with their current level of activity, with no control for social interaction.
Measurements
All measurements were taken in the park, 1 week before the intervention and again 12 weeks later. All measurements were completed on the same specified day, not involving a Tai Chi session for the post-intervention assessment.
Balance was assessed using the Functional Reach Test (FRT). Reach was measured in standardized procedure by attaching a leveled yardstick to a wall with tape at the height of the right acromion process. The subject was asked to stand in a relaxed stance with their shoulders perpendicular to the yardstick, and were instructed not to touch the wall but to extend the elbow with the shoulder at 90° flexion, and hold the position for 3 s. The placement of the third fingertip was recorded (position 1). The subject was then asked to reach as far forward as they could without losing their balance or taking a step, and to hold for 3 s. The end of the third fingertip was recorded as position 2. Functional reach was measured as the difference between positions 1 and 2. Verbal encouragement was provided to maximize performance. The test has a strong correlation between functional reach and the excursion of the center of pressure (Duncan et al., 1990). Test–re-test reliability of functional reach is high [intraclass correlation coefficient (ICC) = 0.81; inter-rater-reliability (IRR) = 0.98]. FRT reflects skill in forward weight shift, reaching and postural control. It is a slow, controlled, dynamic balance task that involves maintaining the center of gravity over the base of support while performing the reach activity, and invokes several aspects of balance, including strength, biomechanics, propriception, vestibular mechanisms and motor planning. In accordance with previous studies (Donahoe et al., 1994), each subject was allowed two practice trials, with two additional test trials as the optimum procedure to allow for subject variability and fatigue. The average of the two test trials was recorded as the score for the FRT. One trained examiner ‘blind’ to the treatment performed all the tests, with verbal encouragement provided to maximize performance.
The average of two blood pressure measurements was recorded from measurements taken in the seated position after the subject has rested for 5 min. Systolic and diastolic blood pressures (SBP/DBP) were recorded ‘blind’ to group by a certified health care assistance using a sphygmo-manometer according to the guidelines established by the American Heart Association (American Heart Association, 1989). All data were analyzed using SPSS Version 10 (Chicago, IL), with change in functional reach, systolic and diastolic blood pressure assessed by one-way analysis of variance (ANOVA) with repeated measures.
RESULTS
Of the 40 participants recruited, three subjects from the Tai Chi group failed to complete the program and three from the control group did not return for the re-evaluation. The compliance rate was high, with a mean of 34 Tai Chi sessions attended (maximum 36), which ranged from 27 to 36 sessions.
Analyses confirmed the absence of any between-group effects in terms of their baseline systolic and diastolic blood pressure, and functional reach test (Student's t-tests; see Table 1).
Baseline (mean ± SD) characteristics of subjects
| Tai Chi group (n = 17) | Control group (n = 17) | p-value | |
|---|---|---|---|
| Age (years) | 47.2 ± 4.07 | 48.4 ± 4.33 | 0.42 |
| Female (%) | 100 | 100 | – |
| Body weight (kg) | 55.3 ± 8.2 | 56.59 ± 6.2 | 0.61 |
| Body height (cm) | 160.7 ± 3.5 | 162.5 ± 4.1 | 0.12 |
| Systolic blood pressure (mmHg) | 122.4 ± 6.6 | 122.6 ± 6.0 | 0.91 |
| Diastolic blood pressure (mmHg) | 80.8 ± 4.2 | 79.2 ± 3.6 | 0.23 |
| Functional reach (cm) | 26.8 ± 2.8 | 27.2 ± 3.1 | 0.88 |
| Tai Chi group (n = 17) | Control group (n = 17) | p-value | |
|---|---|---|---|
| Age (years) | 47.2 ± 4.07 | 48.4 ± 4.33 | 0.42 |
| Female (%) | 100 | 100 | – |
| Body weight (kg) | 55.3 ± 8.2 | 56.59 ± 6.2 | 0.61 |
| Body height (cm) | 160.7 ± 3.5 | 162.5 ± 4.1 | 0.12 |
| Systolic blood pressure (mmHg) | 122.4 ± 6.6 | 122.6 ± 6.0 | 0.91 |
| Diastolic blood pressure (mmHg) | 80.8 ± 4.2 | 79.2 ± 3.6 | 0.23 |
| Functional reach (cm) | 26.8 ± 2.8 | 27.2 ± 3.1 | 0.88 |
Baseline (mean ± SD) characteristics of subjects
| Tai Chi group (n = 17) | Control group (n = 17) | p-value | |
|---|---|---|---|
| Age (years) | 47.2 ± 4.07 | 48.4 ± 4.33 | 0.42 |
| Female (%) | 100 | 100 | – |
| Body weight (kg) | 55.3 ± 8.2 | 56.59 ± 6.2 | 0.61 |
| Body height (cm) | 160.7 ± 3.5 | 162.5 ± 4.1 | 0.12 |
| Systolic blood pressure (mmHg) | 122.4 ± 6.6 | 122.6 ± 6.0 | 0.91 |
| Diastolic blood pressure (mmHg) | 80.8 ± 4.2 | 79.2 ± 3.6 | 0.23 |
| Functional reach (cm) | 26.8 ± 2.8 | 27.2 ± 3.1 | 0.88 |
| Tai Chi group (n = 17) | Control group (n = 17) | p-value | |
|---|---|---|---|
| Age (years) | 47.2 ± 4.07 | 48.4 ± 4.33 | 0.42 |
| Female (%) | 100 | 100 | – |
| Body weight (kg) | 55.3 ± 8.2 | 56.59 ± 6.2 | 0.61 |
| Body height (cm) | 160.7 ± 3.5 | 162.5 ± 4.1 | 0.12 |
| Systolic blood pressure (mmHg) | 122.4 ± 6.6 | 122.6 ± 6.0 | 0.91 |
| Diastolic blood pressure (mmHg) | 80.8 ± 4.2 | 79.2 ± 3.6 | 0.23 |
| Functional reach (cm) | 26.8 ± 2.8 | 27.2 ± 3.1 | 0.88 |
While a single measure of the FRT was used in the analyses, test reliability was confirmed by correlation across the two measurements (Pearson's r = 0.98; p <0.001). In addition, a random sample of 10 subjects from the Tai Chi group were retested the following day to confirm stability of measurement (r = 0.91; p < 0.001).
ANOVA confirmed a significant interaction for groups across time (p < 0.001). Paired comparisons showed a significant improvement [F = 107; degrees of freedom (df) = 32; p < 0.001] in balance for the Tai Chi group (mean change = 7.2 cm; range = 6.0–8.3 cm), with little change for the control group (mean = −0.26 cm; range = −1.2 to 0.7 cm).
Changes in blood pressure for each group are presented in Figure 1.
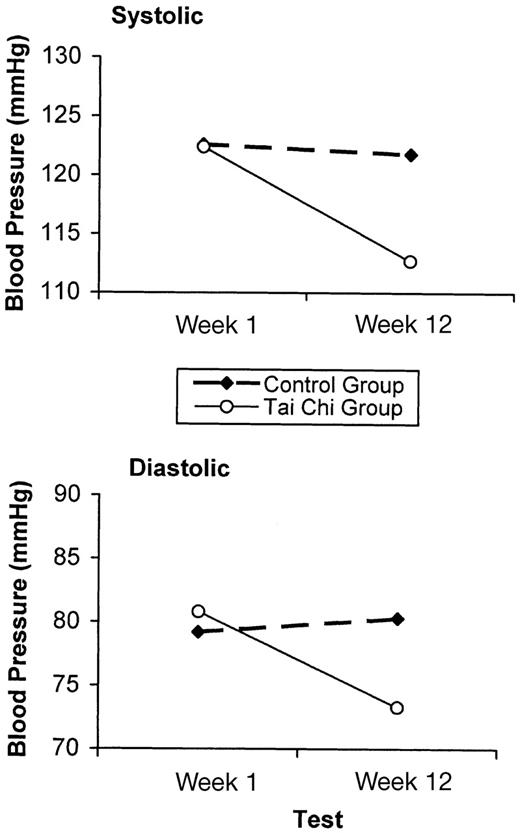
{kind=link}
Group mean systolic and diastolic blood pressure at the beginning and end of the Tai Chi exercise schedule.
Statistical analyses of blood pressure revealed that the Tai Chi group had a significant decrease in both systolic (F = 48.6; p < 0.001; mean decrease = −9.7 mmHg; range = −7.0 to −12.4 mmHg) and diastolic blood pressure (F = 65.6; p < 0.001; mean decrease = −7.5 mmHg; range = −6.0 to −9.0 mmHg). No changes in blood pressure were evident for the control group.
DISCUSSION
The current study provided data to indicate improvement in the dynamic balance of middle-aged persons following a 12-week Tai Chi exercise programme. The programme also resulted in large decreases in blood pressure, which may be of clinical importance given the prognostic implication of elevated pressure for diverse health outcomes later in life.
It has been shown that the practice of Tai Chi exercise can improve balance and reduce falls in elderly individuals (Province et al., 1995; Wolfson et al., 1996; Kutner et al., 1997; Yan, 1998; Wong et al., 2001). However, few studies have indicated benefits for younger age cohorts, with no such published study over recent years. Jacobson and colleagues (Jacobson et al., 1997) and Shih (Shih, 1997) have previously documented improvements in balance, kinesthetic sense and strength in a young and more active population over a period of only 3 months. The studies, however, provide no evidence on dynamic balance or flexibility. Maintaining balance is an ever-changing skill. The integration of highly complex neuromuscular mechanisms is essential to the maintenance of upright posture. The FRT provides a better measurement than that of static balance tests, such as the single leg stance test, which has yielded mixed outcomes in previous studies of Tai Chi (Hong et al., 2000). The mean value of functional reach (33.9 ± 3.9 cm) for the Tai Chi group post-12-week Tai Chi intervention reported here is comparable to that measured in a young (20–40 years) age group (Duncan et al., 1990).
The effect of a Tai Chi programme and other forms of exercise on blood pressure in the elderly has been studied previously [e.g. (Wolf et al., 1996; Young et al., 1999)]. In the study by Young and colleagues, the adjusted mean decreases of systolic blood pressure during a 12-week intervention period were 8.4 and 7.0 mmHg for aerobic exercise and Tai Chi groups, respectively. For diastolic blood pressure, corresponding decreases were 3.2 mmHg in the aerobic exercise group and 2.4 mmHg in the Tai Chi group. These changes in the Tai Chi group for systolic blood pressure are similar to those reported here for relatively sedentary middle-aged individuals and are greater than those reported in the study by Wolf et al. (Wolf et al., 1996). The decreases reported here for diastolic blood pressure are considerably larger than those reported for elderly patients in the study by Young et al. (Young et al., 1999). The data indicate that the potential cardiovascular benefits of Tai Chi may have been underestimated as a result of the previous emphasis on elderly populations (Schaller, 1996). There may be limited potential for blood pressure change in the elderly, especially for diastolic blood pressure which is dependent on elasticity in the arterial wall. At least such a supposition is supported by the changes evident in the middle-age sample in the present study. These data confirm that the benefits of Tai Chi extend beyond balance and flexibility to include cardiovascular measures.
The conclusion of a broad spectrum of benefits is consistent with other statements on Tai Chi [e.g. (Hong and Robinson, 2000)]. The present data suggest benefits are evident in cohorts younger than elderly samples who have provided the focus for previous Tai Chi studies. Health benefits from exercise accrue from maintained activity over a large part of the life-span. Conversely, insults to organ systems from inactivity can occur early in life. Evidence for such statements range through varied conditions, including arteriosclerosis, diabetes and osteoporosis. A continuing challenge in health promotion is to find ‘vehicles’ that increase exercise participation and adherence. Very high levels of adherence as well as positive outcomes were evident in the present study. The high adherence rate confirms that the positive benefits reported cannot be related to self-selection bias through high differential attrition rates in exercise versus control groups that are frequently reported. While there may be variables inherent to Tai Chi that are responsible for such high adherence, including the absence of equipment and a sense of enhanced control, the high adherence rate may be attributed in part to the specific cultural setting.
Tai Chi is a common form of exercise in Hong Kong, and the ‘subjective norm’ — what an individual thinks significant others believe about the value of the exercise — and other ‘social factors’ have become accepted contributing variables in models of exercise adherence (Valois et al., 1988). It is likely therefore that these variables contributed to the high level of adherence. While drop-out rates are high for other forms of exercise in other cultural settings (Dishman, 1988), no direct evidence of the likely drop-out rate for an alternative exercise programme to Tai Chi is available for the population of concern. Consequently, the specific cultural setting and the absence of inclusion of an alternative form of exercise comparison group are limitations of the present study. As such, there remains a question as to the likely uptake of Tai Chi in different ethnic groups and cultural settings. The findings in the present study have been restricted to females, therefore the next question is whether the findings would be replicated for males. Clearly, answers to these questions require further mixed-gender study and extension to different cultural settings.
The present data indicate that for the cohort studied, the positive profiles of change in blood pressure were not significantly related to the improvements in FRT. We are unable to specify whether these vascular decreases are a consequence of the mental or physical relaxation aspects of the exercise since no psychological measure was included in the study. We are also unable to document whether perceived benefits from the programme related to the improved cardiovascular outcome. It is recommended that such measures are included in future studies to elaborate the mechanism for improvements resulting from Tai Chi further.
Despite these limitations, the large and positive outcomes reported in the present study provide support for the wider adoption of Tai Chi as a health promotive activity in younger individuals, and help destroy any stereotype of such activity as an exercise exclusively for benefit in the elderly.
We would like to thank all subjects who agreed to participate in the study.
REFERENCES
American Heart Association (
Brown, D. D., Mucci, W. G., Hetzler, R. K. and Knowlton, R. G. (
Donahoe, B., Turner, D. and Worrell, T. (
Duncan, P. W., Weiner, D. K., Chandler, J. and Studenski, S. (
Ferrucci, L., Benvenuti, E., Bartali, B., Bandinelli, A., DiIorio, A., Ruso, C. R. et al. (
Hong, Y. L., Li, J. X. and Robinson, P. D. (
Jacobson, B. H., Cheng, C. H., Cashel, C. and Guerrero, L. (
Kutner, N. G., Barnhart, H., Wolf, S.L., McNeely, E. and Xu, Z. (
Lai, J. S., Wong, M. K., Lan, C., Chong, C. K., and Lien, I. N. (
Lan, C., Lai, J. S. and Chen, S.Y. (
Leon, A. S., Myers, M. J. and Connett, J. (
Li, F. Z., Harmer, P., McCauley, E., Duncan, T. E., Duncan, S. C., and Chaumeton, N. (
Li, J. X., Hong, Y. and Chan, K. M. (
Province, M. A., Hadley, E. C., Hornbrook, M.C. and Lipsitz, L. A. (
Schaller, K. J. (
Shih, J. (
Stalenhoef, P. A, Diederiks, J. P. M., Knotternus, J. A., Kester, A. D. M. and Crebolder, H. F. J. M. (
Terrio, K. and Auld, G. W. (
Thornton, E.W. (
Valois, P., Desharnais, R. and Godin, G. (
Williams, P and Lord, S. R. (
Wolf, S. L., Barnhart, H. X., Kutner, N. G., McNeely, E., Coogler, C. and Xu, T. (
Wolf, S. L., Barnhart, H. X., Ellison, G. L., and Coogler, C. E. (
Wolf, S. L., Sattin, R. W., O'Grady, M., Freret, N., Ricci, L., Greenspan, A. I. et al. (
Wolfson, L., Whipple, R., Derby, C., Judge, J., King, M., Amerman, P. et al. (
Wong, A. M., Lin, Y. C., Chou, S. W., Tang, F. T. and Wong, P. Y. (
Wu, G. (
Yan, J. H. (
Author notes
1Department of Psychology, University of Liverpool, UK and 2Centre for Exercise Nutrition Science, Chester College, UK