





Abstract
Transmyocardial laser revascularization is an established therapy for refractory coronary artery disease. However, utilization of the technology is not as widespread as expected. This is despite the fact that the efficacy of the technology has been established in multiple prospective randomized trials. Furthermore, only about 5% of transmyocardial laser revascularization cases annually are performed in a minimally invasive fashion. We report a case of a female patient treated in a minimally invasive thoracoscopic fashion.
INTRODUCTION
Coronary artery disease is one of the leading causes of morbidity and mortality. An increasing number of patients have exhausted their non-surgical and surgical treatment options. One approved treatment option for coronary artery disease is transmyocardial laser revascularization (TMR). However, utilization of the technology is not as widespread as expected, despite that the efficacy of the technology has been established in multiple prospective randomized trials [1].
The invasiveness of surgical TMR through a sternotomy or a thoracotomy might be one of the factors leading to a hesitation in usage. We describe our case of performing TMR in a minimally invasive thoracoscopic fashion.
CASE DESCRIPTION
A 46-year-old female presented to us with Class IV angina. Her comorbidities included end-stage kidney disease status post-kidney transplantation with a baseline creatinine of 2.0, obstructive sleep apnoea, diabetes, hypertension, history of transient ischaemic attacks, atrial fibrillation and morbid obesity with a body mass index of 42. She had coronary artery disease in the circumflex distribution, with no options for revascularization (Fig. 1). Coronary angiography showed a patent left anterior descending and right coronary arteries. Echocardiogram showed an ejection fraction of 55%. A positron emission tomography scan showed ischaemia in the lateral wall and the apex. After discussion among the heart team it was decided to proceed with TMR (Video. 1).
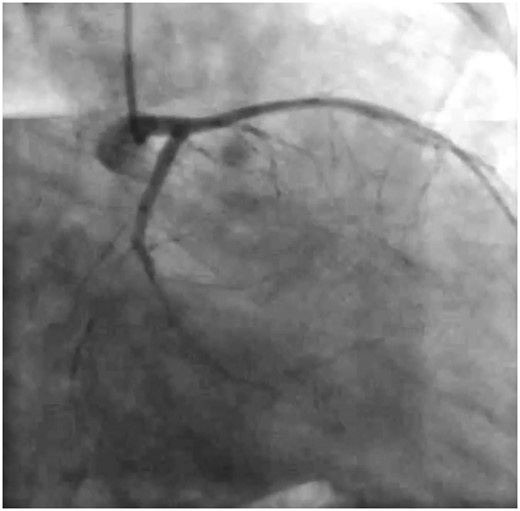
Left coronary angiogram.
Procedural video. Copyright 2015, used with permission from CTSNet (www.ctsnet.org). All rights reserved.
The procedure was performed in the lateral decubitus position with double lumen endotracheal intubation. A camera port was placed in the 8th intercostal space in the posterior axillary line. Under direct vision by the thoracoscope, 2 other 5 mm working ports were placed, 1 anteriorly and the other posteriorly to the pericardial sac. Another optional 10 mm trocar was placed more superiorly, for bleeding control. The chest was insufflated with carbon dioxide to a pressure of 8 mmHg.
The pericardium was opened avoiding the phrenic nerve. Sutures on either side of the pericardium were placed and brought through the chest wall. The anterior, lateral and inferior walls could all be visualized. The laser probe (Holmium YAG laser) was inserted into the anterior 5 mm port. A grasper was used to position the laser probe over the lateral wall and stabilize it while it was passed through the myocardium (Fig. 2). Eleven channels were created in the lateral wall and 3 channels around the apex. On each pass, visualization of bubbles in the left ventricular chamber was confirmed by transoesophageal echocardiography.
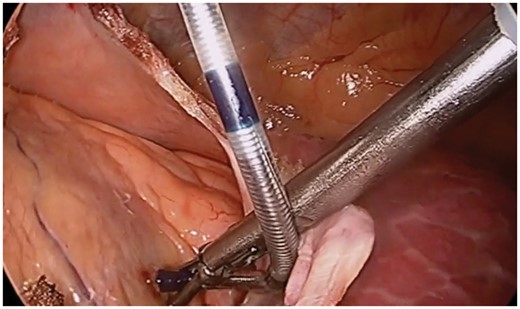
The Pearl 5.0 probe of the Holmium YAG laser positioned with a grasper on the lateral wall.
Patient was discharged on postoperative Day 6 with no symptomatic chest pain or complications. The patient remained angina-free for 3 months. She developed recurrence of angina afterwards, Class I, with an improvement in her activity level.
DISCUSSION
There are approximately 1500 TMR cases done annually using the Holmium laser; only about 5% are done through a minimally invasive approach. The first report of a thoracoscopic TMR using a Holmium laser was published in 1997 [2]. The minimally invasive procedure was described in a technical paper in 1998 [3].
Our technique has the same principle of triangulation of ports; however, we recommend placing the camera port in a lower interspace (the 7th or 8th). This allows better exposure, more room for the surgeon and other instruments. If additional exposure is needed, insufflation of the thoracic cavity can be performed safely; we recommend insufflation up to 8 mmHg. This technique has given us the ability to provide the same number of channels compared to the open approach.
A case series describing 10 patients undergoing thoracoscopic TMR were reported in 2005 [4]. A mean of 30 channels were created, and results showed a significant reduction of angina class from 3.7 to 1.3. The study had a mean follow-up of 8.4 months. This approach might be more challenging in redo surgery situations. However, the procedure can still be done safely, as the adhesion can be taken down thoracoscopically. Allen and Budde [5] described their experience in 17 patients with prior history of coronary artery bypass grafting. A thoracoscopic approach for TMR was possible, with no conversion to thoracotomy. Procedure times, however, were increased with a mean of 27 min.
The thoracoscopic technique results in better pain control, earlier mobilization and earlier discharge. These advantages might lead to less morbidity and mortality, although this has to be validated with randomized trials.
CONCLUSION
Thoracoscopy is a safe and feasible approach to provide TMR therapy. This might lead to higher enthusiasm and better adoption of this unique therapy. Further studies are needed to reproduce these findings and to confirm other benefits regarding the approach.
Conflict of interest: none declared.

{kind=link}
{kind=link}