





Abstract
Gastrointestinal ischemia is caused by ischemic colitis in 50–60% of cases and is associated with high morbidity and mortality among patients. Ischemic proctosigmoiditis is a very rare disorder with only few cases reported. Due to collateral blood supply the rectum is only affected in 2–5% of all cases of ischemic colitis. We report a rare case of ischemic proctosigmoiditis caused by a retroperitoneal hematoma due to a pelvic fracture.
INTRODUCTION
Gastrointestinal ischemia arises due to a sudden reduction in intestinal blood flow, and it most commonly occurs due to mesenteric thrombosis, vasculitis and torsion of the intestine [1]. Intestinal ischemia can arise due to occlusive or non-occlusive disorders. In occlusive conditions, the collateral circuit of the intestine is occluded, which can be seen due to traumas, surgery on aorta or pelvic arteries, or can be caused by thrombosis/embolus in the mesenteric arteries. Non-occlusive conditions are characterized by reduced flow, often due to hypotension such as septic or hypovolemic shock [2]. Ischemia of the intestine causes gangrene and necrosis in the intestinal wall. Mucosal changes occur within ∼20 min to an hour after reduction in blood flow. Transmural ischemia with necrosis will develop within 8–16 h [3].
Ischemic colitis accounts for 50–60% of cases of gastrointestinal ischemia and is associated with a high morbidity and mortality [1]. In contrary, the rectum is only affected in 2–5%, a result of rich collateral blood supply of the rectum [2,4].
Gastrointestinal ischemia often has a vague clinical presentation that resembles many other gastrointestinal disorders. Symptoms include abdominal pain, gastrointestinal bleeding, diarrhea (68%), abdominal distention (63%) and nausea/vomiting (38%) [5]. The disease can even be transient due to non-occlusive disorders, which makes it difficult to find the exact etiology of the ischemia and diagnosis may be delayed while exploring more common etiologies of the symptoms. Risk factors for development of intestinal ischemia include age >65 years, hypertension, renal failure, diabetes, history of irritable bowel disease, chronic obstructive pulmonary disease, constipation and atherosclerosis [6–8].
In this case report, we describe a rare case of ischemic proctosigmoiditis due to retroperitoneal hematomas in a patient with a pelvic fracture.
CASE REPORT
An 87-year-old woman was admitted to the emergency unit due to abdominal pain and diarrhea. Her previous medical history included hypertension and third-degree atrioventricular block treated with pacemaker. She had no previous abdominal surgeries or known gastrointestinal conditions. Prior to admission, the patient had fallen at home and was complaining about dizziness, lower abdominal pain, watery stool for the past 24 h and right-sided pelvic pain. Initial assessment revealed following vital parameters: blood pressure 122/50 mmHg, pulse 63/min, respiratory rate 20/min, saturation 90% on room air and temperature 35.5°C.
During physical examination, the patient complained of tenderness over the pubic bone and lower abdomen, while no peritoneal reaction was found. Right hip region was swollen and tender upon examination. Rectal examination was normal.
Biochemical measures revealed: hemoglobin 6.5 mmol/l (7.3–9.6), white blood cell count 10.6 × 109/l (3.5–8.8), platelets 102 × 109/l (145–390), creatinine 196 µmol/l (50–90) and C-reactive protein 29 mg/l (<8). Arterial blood gas analysis showed pH 7.16 (7.35–7.45) and lactate 13.6 mmol/l (0.5–1.6).
X-ray of the pelvic region revealed a right-sided nondisplaced pubic ramus fracture.
After 9 h, the arterial blood gas was repeated and showed pH 7.42 and lactate 2.7. Due to near normalization of blood gas parameters upon i.v. fluid administration, the pelvic fracture was believed to be caused by a fall due to severe dehydration and diarrhea.
Twenty-one hours after admission, the patient’s condition worsened and she was complaining of severe abdominal pain. C-reactive protein increased to 123 mmol/l. A suspicion of intestinal ischemia arose, and without further radiologic examination, the patient was taken to the operating room for exploratory laparotomy. Intra-operatively, necrosis of the sigmoid colon and proximal part of rectum were detected. Flexible sigmoidoscopy revealed non-vital mucosa 10–25 cm from anus. Additionally, another 10 cm area of non-vital ileum was detected 20 cm from the ileocecal region, which were adherent to the rectosigmoid junction. Retroperitoneal hematomas were detected in the pelvic region, while no hematoma was identified in proximity to the inferior mesenteric artery. All non-vital intestinal segments were resected, and ileostomy and sigmoideostomy were performed. Only minor bleeding was encountered during the procedure. Postoperatively, the patient had severe sepsis and was kept at the intensive care unit. However, she recovered and was discharged 10 days after admission.
Histopathology of the resected tissue showed necrosis due to ischemia without any sign of vasculitis or thrombosis (Fig. 1).
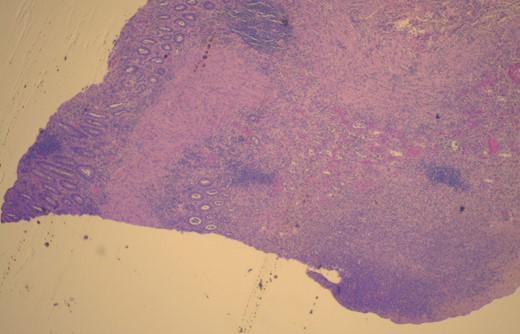
Micrograph of resected colon. Histopathologic analysis showing necrotic colon with transmural necrosis. Hematoxylin and eosin stain.
DISCUSSION
We report a rare case of acute ischemic proctosigmoiditis where the origin of ischemia is difficult to establish. Previously, only a few cases of ischemic proctitis have been reported in patients with pelvic fractures due to high-energy traumas, but no previous reports on ischemic proctosigmoiditis have been reported [9,10].
The blood supply to the sigmoid colon arises from the inferior mesenteric artery through the sigmoid artery and its end branch, the superior rectal artery [1]. The rectum has a rich blood supply which originates from the superior rectal artery and the middle and distal rectal artery, branches of the paired internal iliac artery. In addition, there is abundant collateral blood supply to the distal colon and rectum from the marginal artery of Drummond that links the superior and inferior mesenteric arteries [1,2].
In this case, we report ischemia of the distal part of sigmoid colon and proximal part of rectum. This is an atypical location of ischemia due to the rich collateral blood supply. However, this patient had increased age, known hypertension and cardiovascular disease that could explain the increased susceptibility to ischemia. We assume that the origin of ischemia in this case was a pelvic fracture that caused retroperitoneal hematomas resulting in a local increase in retroperitoneal pressure and obstruction of the blood supply to the affected part of rectum and colon sigmoideum. Subsequently, ischemia and necrosis have occurred. Possibly, early computed tomography imaging could have identified an expanding retroperitoneal hematoma and thus allowed for embolization by interventional radiologists.
Ischemia of colon and rectum are serious conditions associated with high morbidity and a mortality of 40% in patients with transmural necrosis of the rectum [2]. This emphasizes the need for early diagnosis, management and possible surgical intervention. Our case illustrates that ischemia of the intestinal wall can arise due to pelvic fractures in patients with risk factors for vessel disease, and clearly states the difficulty in placing the correct diagnose of gastrointestinal ischemia.
CONFLICT OF INTEREST STATEMENT
None declared.
ACKNOWLEDGEMENTS
The authors would like to thank Dr Matteo Biagini, Department of Histopathology, Roskilde University Hospital, for providing histopathologic micrograph and description.

{kind=link}