





Abstract
Objective. Gua sha is a traditional East Asian healing technique where the body surface is press-stroked with a smooth-edged instrument to intentionally raise therapeutic petechiae. A traditional indication of Gua sha is neck pain; no data from controlled trials exist to support this claim. The researchers aimed to investigate the effectiveness of Gua sha in the symptomatic treatment of chronic neck pain.
Design. The study was designed as an open randomized controlled clinical trial.
Setting. The study was set in Kliniken Essen-Mitte, Academic Teaching Hospital of the University Duisburg-Essen, Germany.
Subjects. Forty-eight outpatients (58.5 ± 8.0 years; 41 female) with chronic mechanical neck pain were the subjects of the study.
Intervention. Patients were randomized into Gua sha (N = 24) or control groups (N = 24) and followed up for 7 days. Gua sha patients were treated once with Gua sha, while control patients were treated with a local thermal heat pad.
Outcome Measures. Primary outcome was change of neck pain severity after 1 week as assessed by visual analog scale. Secondary outcomes included pain at motion, the neck disability index (NDI) and quality-of-life (Short-Form [36] Health Survey).
Results. Neck pain severity after 1 week improved significantly better in the Gua sha group compared with the control group (group difference −29.9 mm, 95% confidence interval: −43.3; −16.6 mm; P < 0.001). Significant treatment effects were also found for pain at motion, scores on the NDI, and dimensions of quality-of-life. The treatment was safe and well tolerated.
Conclusion. Gua sha has beneficial short-term effects on pain and functional status in patients with chronic neck pain. The value of Gua sha in the long-term management of neck pain and related mechanisms remains to be clarified.
Introduction
Chronic neck pain is a common medical complaint with a high socioeconomic impact. Recent studies estimate its point prevalence to be between 6% and 22%, which increases with age [1–3]. Twelve-month prevalence is estimated to amount to 30–50% [1]. Suffering from neck pain is very costly because of increased demand for health care [4].
Chronic neck pain can be caused by the dysfunction of a variety of structures in the neck [5]. Often, symptoms persist, causing a substantial deterioration in the quality-of-life and a substantial loss of work time [6]. Conventional conservative treatment options comprise exercise, massage, physical therapy, education, local anesthetic infiltration, and systemic drug use. There are systematic reviews for many treatment modalities; however, there is still a lack of evidence for most therapies [7], and a multimodal approach is increasingly favored [8]. Evidence for the effectiveness of nonsteroidal anti-inflammatory drugs (NSAIDs), which are still a mainstay of conservative treatment, are contradictory while their adverse effects are well known [9]. Because standard treatments for chronic neck pain are less than satisfactory, other conservative methods, including those from traditional medicine, should be further evaluated.
A recent systematic review found moderate evidence for the pain-relieving effect of acupuncture [10]. Beside acupuncture, Gua sha is another essential modality of traditional Asian medicine. Gua sha may be defined as instrument-assisted unidirectional “press-stroking” of a lubricated area of the body surface that intentionally creates transitory therapeutic petechiae representing extravasation of blood in the subcutis [11]. Gua sha has been used for centuries in Asia [12,13], in Asian immigrant communities [14,15] and by acupuncturists and practitioners of traditional East Asian medicine worldwide [10,16–19]. With the expansion of traditional Asian medicine, Gua sha has been used over broad geographic areas and by millions of people. Gua sha is commonly applied for regional pain and for functional problems with impaired movement [16,18]. A 2005 search of Chinese medical literature identified 120 studies on Gua sha, especially for painful musculoskeletal conditions. One quarter of the articles reported on Gua sha were related to neck disorders[17,20].
However, a systematic review of controlled trials conducted in China found favorable effects of Gua sha on pain reduction in several trials but concluded that evidence was insufficient because of poor methodological quality [21]. The Western medical literature reports one randomized controlled trial demonstrating Gua sha to be effective for breast engorgement [22]. Moreover, there are case reports in the Western literature for Gua sha in the treatment of pain [23,24], as well as studies on the physiology of Gua sha; specifically showing a significant increase in surface microperfusion [11] as well as upregulation of gene expression of hemo-oxygenase-1(HO-1) subsequent to Gua sha [25]. According to traditional Chinese medicine, Gua Sha removes stasis (sha) in affected tissues.
To date, there has been no randomized trial in the Western literature evaluating the effectiveness of Gua sha for musculoskeletal pain. The researchers therefore designed this randomized pilot study to evaluate whether Gua sha is beneficial for acute relief in chronic neck pain.
The researchers hypothesized that a single Gua sha treatment leads to significantly reduced neck pain severity compared with a thermal control therapy after 1 week.
Methods
This study was designed as a randomized controlled open trial. All study participants gave their informed consent. The study protocol was reviewed and approved by the Ethics Committee of the Medical Faculty, University of Duisburg-Essen, Germany. All study procedures and the collection of data was carried out at the outpatient department of the Kliniken Essen-Mitte, an academic teaching hospital of the University of Duisburg-Essen, Germany.
Study Procedures
The researchers recruited participants by means of a press release offering participation in a study of complementary medicine for chronic neck pain. Potential participants were screened for eligibility by telephone interview, and eligible candidates were scheduled for enrolment visits. A study physician performed the candidates' physical examinations, and measures were administered by a trained and blinded research staff. Thereafter, each eligible participant was randomly assigned to either the Gua sha or a control group, and the respective treatment started. All measures were repeated on Day 7 after the allocated treatment. The written and personal study information emphasized that both treatments might be useful for treatment of chronic neck pain.
Study Participants
Patients of both sexes were eligible if they were between 18 and 70 years old and were suffering from a minimum neck pain score of 30 mm on a 100-mm visual analog scale (VAS) and a self-reported painful restriction of cervical spine mobility for at least 3 months.
Subjects were excluded if they had undergone invasive treatment within the previous month, were receiving anticoagulants or had hemophilia, anemia, skin disease in the region of treatment, or a coexisting serious illness. The researchers also excluded patients if they were participating in another study, had previously experienced treatments with Gua sha or the ginger heat pad, or if they had undergone previous surgery in the neck region or had a manifest neurological deficit. Subjects regularly taking NSAIDs or analgesics as rescue medication were not excluded if the mean weekly dosage and type of administration had not been altered during the preceding 3 months.
Randomization
Patients were randomly allocated to a treatment group by a nonstratified block randomization with varying block lengths and by preparing sealed, sequentially numbered opaque envelopes containing the treatment assignments. Randomization was based on the “ranuni” pseudo-random number generator of the SAS/Base® statistical software (SAS Inc., Cary NC, USA), and the envelopes were prepared by the study biostatistician. When a patient fulfilled all enrolment criteria, the study physician opened the lowest numbered envelope to reveal that patient's assignment.
Treatment Protocols
Subjects were treated once with either Gua sha or a heat pad on the day of their baseline data collection. Both treatments were carried out by two experienced therapists. All subjects were allowed to continue their existing medication. Subjects in the control group were offered a free Gua sha massage on follow-up 1 week later (waiting list offer) to reduce nocebo effects. All subjects were told to keep warm and abstain from heavy physical activities for the rest of the day of their treatment. Both treatments lasted approximately 30 minutes.
Gua Sha Intervention
Gua sha was delivered to the upper back and entire neck by a standard protocol irrespective of the hurting area. Subjects were treated in a seated position. Gua sha was performed by trained therapists using a small lid with a rounded edge and a skin lubricant (Tumarol®, Robugen Pharmazeutische Fabrik GmbH, Esslingen Germany) to decrease friction. Following a diagnostic palpation demonstrating the presence of “sha” stasis (pressing of fingers on the skin resulting in blanching that is slow to fade) indicating the need for Gua sha, the back and neck were press-stroked in sequential stroke areas until no further Sha (petechiae) could be raised.
Control Treatment
Because of the specific nature of Gua sha, there can be no ideal sham treatment. The researchers therefore considered well-accepted treatment modalities with beneficial short-term effects as control interventions. A thermal treatment was chosen because in Germany, locally applied heat is well accepted by patients. Evidence from randomized clinical trials documenting the efficacy of locally applied heat in chronic pain conditions is limited [26]. However, local heat causes vasodilation, increases analgesia, and reduces muscle spasm, which would support its use in patients with chronic pain conditions [27,28].
Furthermore, we chose a specific heat pad (“Zappsack,” Fa COOC, Bönen, Germany) with an ingredient from Chinese medicine (dried ginger) and patients were told that the heat pad showed promising effects in chronic neck pain. In Chinese medicine, external ginger is used to enhance the subjective feeling of warmth. The heat pad was applied once for 15–20 minutes to the neck with the patient in seated position.
To adjust for unspecific effects, we selected the treatment duration to be roughly equal to that of Gua sha. It was furthermore carried out by the same two practitioners as Gua sha and the therapist stayed throughout the control intervention.
All subjects were asked to complete standardized questionnaires at the outset of the study (baseline, Day 0) and after 1 week (Day 7) in the study center. Average neck pain intensity (irrespective of movement) during the 1-week study period was assessed on a VAS daily, where 0 means no pain and 100 maximum pain. The primary outcome measure was change in neck pain severity from Day 0 to Day 7 as derived from the VAS.
Subjects further completed the Neck Disability Index (NDI), a validated disease-specific quality-of-life measurement [29]. The NDI consists of 10 questions, each scaled on a 5-point Likert scale, that mainly focus on the physical aspects of neck pain disability [30]. The NDI summary score ranges from 0 to 100 with higher scores indicating higher disability. It has been shown to be one-dimensional, valid and reliable in a 1 week follow-up.
In addition, subjects scored the neck pain at motion (pain related to movement) at study Days 0, 1, and 7 by means of six 100-mm VAS asking for the perceived pain when moving the head in different directions (up, down, turning left, turning right, tilting left, tilting right). Subjects were asked to mark their maximum pain on a given VAS. Secondary outcomes included the mean and the maximum pain of these scales.
Secondary outcomes included the health-related quality-of-life measured by the Short-Form (36) Health Survey (SF-36) [31]. The SF-36 summary scales (physical and mental quality-of-life) have previously been shown to detect differences and changes in the functional status of neck pain patients just as well as the NDI [32]. They were scaled such that the German norm population has a mean score of 50 and a standard deviation (SD) of 10. Higher scores indicate better quality-of-life.
At baseline we documented sociodemographic and clinical characteristics. To control for nonspecific effects of treatment, subjects were asked to rate their expected outcomes before random assignment on a 100-mm VAS. Further, subjects were asked after 1 week how much they had overall profited from their respective treatment on a 100-mm VAS and if they would undergo treatment again.
Adverse effects were assessed by prespecified lists to be filled in by the study physician. Additionally, subjects were asked to keep a diary from Day 0 to 7, recording any adverse effects of their treatment and their use of oral rescue medication. Trained, un-blinded research assistants collected patient-reported data, and research personnel blinded to group allocation entered and monitored the data.
Sample Size Determination and Statistical Analysis
The study was powered to detect a change of 20 mm on the main outcome criterion between both treatment groups with 80% power on the basis of a SD of 24 mm and a two-sided significance level of α = 5%. This yielded a total of 48 subjects.
All outcome criteria were analyzed by intention-to-treat, including all randomized subjects, irrespective whether or not they adhered to the protocol or gave a full set of data. Missing values were multiply imputed [33], i.e., multiple copies of the original data set were generated, hereby replacing missing values by randomly generated values. Each copy (now containing a complete set of data) was analyzed separately and the results were adequately combined.
Data at Day 7 were analyzed by simple analyses of covariance (ancova), which took group as a between-subject factor, and the respective baseline value as a linear covariate. Treatment effects were estimated within these models and reported as adjusted mean differences, including respective 95% confidence intervals (CIs) and P-values from adequate two-sided t-tests. Supplementary analyses were done to adjust for the effects of possibly confounding variables (age, body mass index) and namely outcome expectation. Here, we added these variables as covariates to the ancova models and estimated the group differences in the presence of these covariates.
Results
Between December 2006 and April 2007, 48 subjects were recruited into the trial. Of the 48 subjects randomly assigned to one of the two study groups, four withdrew from the study after treatment and were lost to 7-day follow-up (Figure 1). Three subjects in the Gua sha group were unwilling to return for further visits to the study center and withdrew from the study immediately after Day 1. At a telephone interview they reported that they were satisfied with the study procedures and that they did not experience any adverse effects. One patient in the control group withdrew from the study after randomization seeking other treatments for his neck pain.
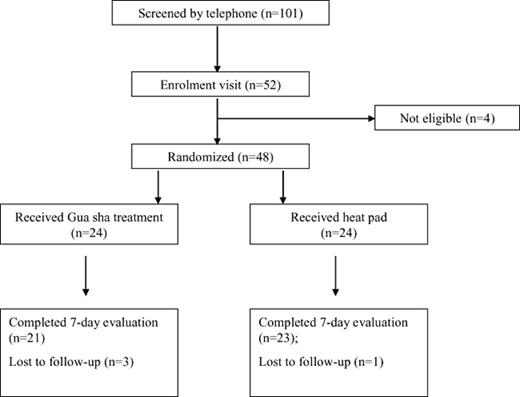
CONSORT trial flowchart.
Baseline Data
Baseline characteristics were well balanced between both groups (Table 1). Subjects in the thermal therapy group were nonsignificantly older than subjects in the Gua sha group. Mean duration of illness was about 8 years in both groups. All secondary and primary outcome measures showed no significant differences at baseline. Quality-of-life-scores were nearly 0.5 SDs below norm for most items regardless of treatment group at baseline. Likewise, the NDI revealed a similar level of disability for both groups at baseline. There was no significant difference between the groups regarding the treatment expectation at baseline (P = 0.170).
Baseline characteristics of study patients
| Characteristic | Gua sha Therapy (N = 24) | Thermal Therapy (N = 24) |
| Age (years) | 45.9 ± 12.2 | 53.0 ± 11.8 |
| male/female | 5/19 | 2/22 |
| Mean duration of symptoms ± SD (years) | 8.4 ± 5.7 | 8.1 ± 6.5 |
| Mean body mass index ± SD (kg/m2) | 23.9 ± 4.7 | 22.5 ± 3.2 |
| Mean weight ± SD (kg) | 73.8 ± 13.6 | 65.0 ± 13.4 |
| Mean NDI score* ± SD (0 to 100) | 32.8 ± 11.5 | 35.6 ± 11.0 |
| Mean neck pain at rest ± SD,* (0 to 5) | 2.5 ± 9.7 | 2.3 ± 0.8 |
| Mean SF-36 physical quality of life ± SD | 41.8 ± 7.9 | 41.2 ± 9.8 |
| Mean SF-36 mental quality-of-life ± SD | 42.8 ± 12.7 | 41.6. ± 12.0 |
| Mean outcome expectation | 76.5 ± 20.8 | 67.1 ± 22.3 |
| Characteristic | Gua sha Therapy (N = 24) | Thermal Therapy (N = 24) |
| Age (years) | 45.9 ± 12.2 | 53.0 ± 11.8 |
| male/female | 5/19 | 2/22 |
| Mean duration of symptoms ± SD (years) | 8.4 ± 5.7 | 8.1 ± 6.5 |
| Mean body mass index ± SD (kg/m2) | 23.9 ± 4.7 | 22.5 ± 3.2 |
| Mean weight ± SD (kg) | 73.8 ± 13.6 | 65.0 ± 13.4 |
| Mean NDI score* ± SD (0 to 100) | 32.8 ± 11.5 | 35.6 ± 11.0 |
| Mean neck pain at rest ± SD,* (0 to 5) | 2.5 ± 9.7 | 2.3 ± 0.8 |
| Mean SF-36 physical quality of life ± SD | 41.8 ± 7.9 | 41.2 ± 9.8 |
| Mean SF-36 mental quality-of-life ± SD | 42.8 ± 12.7 | 41.6. ± 12.0 |
| Mean outcome expectation | 76.5 ± 20.8 | 67.1 ± 22.3 |
SD = standard deviation; NDI = Neck Disability Index; SF-36 = Short-form 36 health survey, population adjusted score.
Derived from neck pain disability index. No significant group differences with exception of weight (P = 0.023). Group difference for age, P = 0.051.
Baseline characteristics of study patients
| Characteristic | Gua sha Therapy (N = 24) | Thermal Therapy (N = 24) |
| Age (years) | 45.9 ± 12.2 | 53.0 ± 11.8 |
| male/female | 5/19 | 2/22 |
| Mean duration of symptoms ± SD (years) | 8.4 ± 5.7 | 8.1 ± 6.5 |
| Mean body mass index ± SD (kg/m2) | 23.9 ± 4.7 | 22.5 ± 3.2 |
| Mean weight ± SD (kg) | 73.8 ± 13.6 | 65.0 ± 13.4 |
| Mean NDI score* ± SD (0 to 100) | 32.8 ± 11.5 | 35.6 ± 11.0 |
| Mean neck pain at rest ± SD,* (0 to 5) | 2.5 ± 9.7 | 2.3 ± 0.8 |
| Mean SF-36 physical quality of life ± SD | 41.8 ± 7.9 | 41.2 ± 9.8 |
| Mean SF-36 mental quality-of-life ± SD | 42.8 ± 12.7 | 41.6. ± 12.0 |
| Mean outcome expectation | 76.5 ± 20.8 | 67.1 ± 22.3 |
| Characteristic | Gua sha Therapy (N = 24) | Thermal Therapy (N = 24) |
| Age (years) | 45.9 ± 12.2 | 53.0 ± 11.8 |
| male/female | 5/19 | 2/22 |
| Mean duration of symptoms ± SD (years) | 8.4 ± 5.7 | 8.1 ± 6.5 |
| Mean body mass index ± SD (kg/m2) | 23.9 ± 4.7 | 22.5 ± 3.2 |
| Mean weight ± SD (kg) | 73.8 ± 13.6 | 65.0 ± 13.4 |
| Mean NDI score* ± SD (0 to 100) | 32.8 ± 11.5 | 35.6 ± 11.0 |
| Mean neck pain at rest ± SD,* (0 to 5) | 2.5 ± 9.7 | 2.3 ± 0.8 |
| Mean SF-36 physical quality of life ± SD | 41.8 ± 7.9 | 41.2 ± 9.8 |
| Mean SF-36 mental quality-of-life ± SD | 42.8 ± 12.7 | 41.6. ± 12.0 |
| Mean outcome expectation | 76.5 ± 20.8 | 67.1 ± 22.3 |
SD = standard deviation; NDI = Neck Disability Index; SF-36 = Short-form 36 health survey, population adjusted score.
Derived from neck pain disability index. No significant group differences with exception of weight (P = 0.023). Group difference for age, P = 0.051.
Outcome Measures
Primary Outcome
Gua sha therapy was more beneficial than thermal therapy with regard to neck pain intensity at Day 7. The mean (±SD) pain score was reduced from 61.3 ± 14.0 mm to 22.2 ± 22.3 mm in the Gua sha group and from 58.3 ± 16.2 mm to 50.3 ± 23.4 mm in the control group with a highly significant between-group difference of −29.9 mm (95% CI: −43.3; −16.6; P < 0.001, ancova). Similar results were obtained when outcome expectation was included as an additional factor (group difference −31.5 mm; 95% CI: −47.7; −15.2, P = 0.001). Average daily pain scores, obtained from the diaries, showed an immediate pain relief by Gua sha which was sustained during the 1-week study period (Figure 2).
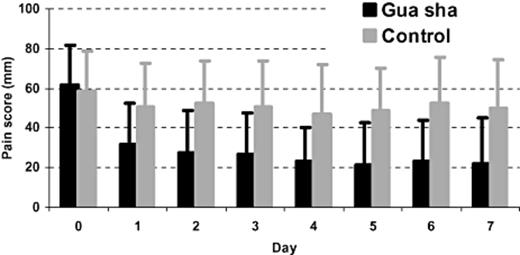
Pain score. Means ± standard deviation of the visual analog scale pain score in the Gua sha and the control intervention groups during the 7-day course of the study.
Significant group differences favoring Gua sha therapy over thermal therapy were also found in the NDI (Table 2). Pain at motion was also improved significantly by Gua sha in five of the six motion categories resulting in significant group differences favoring Gua sha for mean pain at motion and maximum pain at motion (Table 2).
NDI and neck pain related to movement
| Neck Disability Index | Baseline | Day 1 | Day 7 | Group Difference Baseline—Day 7 Mean (95% CI) | P-value |
| NDI sum score | |||||
| Gua sha therapy | 32.8 ± 11.5 | 21.8 ± 12.9 | −8.5 (−13.6; −3.5) | <0.001 | |
| Thermal therapy | 35.6 ± 11.0 | 32.8 ± 12.5 | |||
| Mean pain related to motion | |||||
| Gua sha therapy | 50.6 ± 24.1 | 29.2 ± 24.0 | 24.7 ± 24.4 | −23.5 (−34.5; −12.5) | <0.001 |
| Thermal therapy | 51.0 ± 19.4 | 45.7 ± 23.9 | 47.1 ± 23.5 | ||
| Maximum pain related to motion | |||||
| Gua sha therapy | 67.8 ± 22.8 | 44.1 ± 32.0 | 36.4 ± 31.2 | −19.1 (−31.7; −6.6) | <0.003 |
| Thermal therapy | 68.3 ± 19.3 | 60.1 ± 24.2 | 60.3 ± 23.7 |
| Neck Disability Index | Baseline | Day 1 | Day 7 | Group Difference Baseline—Day 7 Mean (95% CI) | P-value |
| NDI sum score | |||||
| Gua sha therapy | 32.8 ± 11.5 | 21.8 ± 12.9 | −8.5 (−13.6; −3.5) | <0.001 | |
| Thermal therapy | 35.6 ± 11.0 | 32.8 ± 12.5 | |||
| Mean pain related to motion | |||||
| Gua sha therapy | 50.6 ± 24.1 | 29.2 ± 24.0 | 24.7 ± 24.4 | −23.5 (−34.5; −12.5) | <0.001 |
| Thermal therapy | 51.0 ± 19.4 | 45.7 ± 23.9 | 47.1 ± 23.5 | ||
| Maximum pain related to motion | |||||
| Gua sha therapy | 67.8 ± 22.8 | 44.1 ± 32.0 | 36.4 ± 31.2 | −19.1 (−31.7; −6.6) | <0.003 |
| Thermal therapy | 68.3 ± 19.3 | 60.1 ± 24.2 | 60.3 ± 23.7 |
NDI = Neck Disability Index.
NDI sum scores in both study groups at baseline and Day 7 with group differences for change on treatment. Sum scores for mean and maximum Pain related to movement in six directions at baseline, at Day 1 and Day 7 after treatment in both study groups as well as group differences for change on treatment between baseline and Day 7.
NDI and neck pain related to movement
| Neck Disability Index | Baseline | Day 1 | Day 7 | Group Difference Baseline—Day 7 Mean (95% CI) | P-value |
| NDI sum score | |||||
| Gua sha therapy | 32.8 ± 11.5 | 21.8 ± 12.9 | −8.5 (−13.6; −3.5) | <0.001 | |
| Thermal therapy | 35.6 ± 11.0 | 32.8 ± 12.5 | |||
| Mean pain related to motion | |||||
| Gua sha therapy | 50.6 ± 24.1 | 29.2 ± 24.0 | 24.7 ± 24.4 | −23.5 (−34.5; −12.5) | <0.001 |
| Thermal therapy | 51.0 ± 19.4 | 45.7 ± 23.9 | 47.1 ± 23.5 | ||
| Maximum pain related to motion | |||||
| Gua sha therapy | 67.8 ± 22.8 | 44.1 ± 32.0 | 36.4 ± 31.2 | −19.1 (−31.7; −6.6) | <0.003 |
| Thermal therapy | 68.3 ± 19.3 | 60.1 ± 24.2 | 60.3 ± 23.7 |
| Neck Disability Index | Baseline | Day 1 | Day 7 | Group Difference Baseline—Day 7 Mean (95% CI) | P-value |
| NDI sum score | |||||
| Gua sha therapy | 32.8 ± 11.5 | 21.8 ± 12.9 | −8.5 (−13.6; −3.5) | <0.001 | |
| Thermal therapy | 35.6 ± 11.0 | 32.8 ± 12.5 | |||
| Mean pain related to motion | |||||
| Gua sha therapy | 50.6 ± 24.1 | 29.2 ± 24.0 | 24.7 ± 24.4 | −23.5 (−34.5; −12.5) | <0.001 |
| Thermal therapy | 51.0 ± 19.4 | 45.7 ± 23.9 | 47.1 ± 23.5 | ||
| Maximum pain related to motion | |||||
| Gua sha therapy | 67.8 ± 22.8 | 44.1 ± 32.0 | 36.4 ± 31.2 | −19.1 (−31.7; −6.6) | <0.003 |
| Thermal therapy | 68.3 ± 19.3 | 60.1 ± 24.2 | 60.3 ± 23.7 |
NDI = Neck Disability Index.
NDI sum scores in both study groups at baseline and Day 7 with group differences for change on treatment. Sum scores for mean and maximum Pain related to movement in six directions at baseline, at Day 1 and Day 7 after treatment in both study groups as well as group differences for change on treatment between baseline and Day 7.
The physical quality-of-life showed a trend toward a beneficial effect of Gua sha (P = 0.055), as well as the subscales for vitality (P = 0.056), general health perception (P = 0.054), and mental health (P = 0.078). Physical function was significantly improved by Gua sha (mean difference 4.2 [95% CI: 7.1; 1.4: P = 0.036]) as well as the subscale social function (mean difference 6.5 [95% CI: 12.4; 0.7: P = 0.0278]).
Global patient rating at the end of study revealed higher patient satisfaction with Gua sha compared with control intervention (55.7 ± 33 mm vs 26.9 ± 28.7 mm; P = 0.016, Wilcoxon test). Finally, the use of oral analgesics was comparable and was rare in both groupsthroughout the study period with no significant differences between the groups.
In general, higher outcome expectation was not associated with study outcome and statistical adjustment of the treatment effects for baseline outcome expectation did not affect the overall results. Thus, there was no indication that outcome was largely affected by the subjects' expectations.
Safety
There were no serious adverse events in either study group. Regular minor adverse effects were related to the appearance of petechiae at the sites of application of Gua sha. Other minor adverse effects were reported by 25% of subjects in the Gua sha group and 21% of subjects in the thermal group. They included mainly slight muscle aches and soreness in the area of treatment.
Discussion
Chronic neck pain is highly prevalent in European populations [1–3]. Because conservative options for treatment are limited, new therapeutic approaches need to be considered. Gua sha, a traditional treatment modality from East Asian medicine, is widely used in Asia for symptom relief in neck pain. Expert opinion and Chinese literature point to its effectiveness in chronic neck pain [11,17,20]. However, no studies have been done in a Western population.
In this randomized controlled trial, subjects with chronic neck pain who were treated once with Gua sha experienced a rapid and highly significant decrease in neck pain and improvement of neck pain disability. The symptomatic improvement was sustained in the short-term study observation period of 1 week. Furthermore, Gua sha therapy, as applied in this study and despite producing transitory impressive skin petechiae and ecchymosis, was safe and well tolerated by all treated subjects.
According to recent consensus statement, pre–post treatment changes of approximately 20 mm using a 100-mm VAS represent the patient feeling “much better” or “meaningfully” improved, and a decrease of ≥4 points or ≥50% appears to represent their feeling substantially (“very much”) improved [34]. In this trial, the mean of the pain score decreased by 39 mm and more than 50%, reflecting a clinically meaningful improvement.
The strengths of this study include the randomized study design, qualified Gua sha therapists, validated outcome measures, and the presence of a control group.
A limitation of our study is that it is a single-blinded trial and treatment as well as therapists were not blinded to group assignments. Therefore, the placebo-like and unspecific treatment effects cannot be well controlled and precisely assessed. So far, it has not been possible to blind for procedures like Gua sha, which entails very specific skin pressure and leads to prominent and visible petechiae. For these reasons we decided to assess the effectiveness of Gua sha in an open trial and to use a well-accepted control intervention. Because the effect of the Gua sha intervention in a population with chronic neck pain was large, it seems unlikely that it can be fully explained by unspecific effects with non-blinding. Furthermore, we assessed outcome expectation in order to approximate the placebo-like effect. Here, the scores did not indicate that the Gua sha group had higher expectations at baseline, and the overall results were not affected by adjustment for the confounding effect of outcome expectation. However, future trials should try to compare Gua sha with similar interventions that use less pressure and do not result in ecchymoses to allow better discrimination of specific effects.
A further limitation of our study is its brief duration. However, we did show that Gua sha results in rapid and clinically relevant symptomatic relief.
In clinical practice, Gua sha is easy to perform and is thus suitable for repetitive treatments. Further studies are now needed to assess the long-term value of Gua sha in the management of chronic neck pain.
Various mechanisms can be considered to explain the observed effect in neck pain. First, nociceptive activation contributes to chronic pain [35], and Gua sha may alleviate pain by means of anti nociceptive effects and by counterirritation [24]. However, at present, it is unclear to what extent Gua sha induces such mechanisms.
Second, a significant increase in surface microperfusion [11] as well as upregulation of gene expression of HO-1 at multiple internal organ sites subsequent to one Gua sha treatment have been established [25]. Still, it remains unclear if these effects also have an impact on chronic neck pain. Of note, traditional cupping therapy has similarities to Gua sha regarding its body surface application and the transitory therapeutic petechiae. Recently, two studies have shown cupping therapy to be efficacious in two regional pain syndromes: low back pain and brachialgia [36,37].
Third, Gua sha therapy may have a powerful placebo effect. In fact, all invasive or nonpharmacological treatments have relevant placebo-like effects. In a recent randomized trial, a sham device was more effective in relieving pain than a placebo pill [38]. Therefore, the nonspecific and placebo-like effects of Gua sha therapy may be augmented from its being an uncommon procedure. But, this is relevant only if placebos are indeed effective in treating chronic pain syndromes, which is still open to discussion [39].
The therapeutic effect of Gua sha may seem greater because of the limited effect of the control treatment to which it was compared. Chronic neck pain is commonly treated with local heat in Germany. However, in this study, we did not repeat the thermal treatment serially as is often performed. Of note, in a recent systematic review, Vernon et al. analyzed the outcome of control groups in clinical trials of conservative treatments for chronic neck pain. They found changes in pain scores of control groups to be similarly small and not to increase over long-term follow-up [40].
In conclusion, a single treatment of Gua sha significantly decreased pain intensity and improved disability for up to 1 week in patients with chronic neck pain as compared with patients receiving thermal therapy. Gua sha is safe, simple to apply, and inexpensive. The effects of this treatment and its related mechanisms should be further investigated in randomized trials of longer duration using other or similar treatments as controls.
Acknowledgments
The study was supported by the Karl and Veronica Carstens Foundation, Germany.
References

{kind=link}
{kind=link}