





Abstract
Objectives. The objective of this study was to estimate the societal costs of prescription opioid abuse, dependence, and misuse in the United States.
Methods. Costs were grouped into three categories: health care, workplace, and criminal justice. Costs were estimated by 1) quantity method, which multiplies the number of opioid abuse patients by cost per opioid abuse patient; and 2) apportionment method, which begins with overall costs of drug abuse per component and apportions the share associated with prescription opioid abuse based on relative prevalence of prescription opioid to overall drug abuse. Excess health care costs per patient were based on claims data analysis of privately insured and Medicaid beneficiaries. Other data/information were derived from publicly available survey and other secondary sources.
Results. Total US societal costs of prescription opioid abuse were estimated at $55.7 billion in 2007 (USD in 2009). Workplace costs accounted for $25.6 billion (46%), health care costs accounted for $25.0 billion (45%), and criminal justice costs accounted for $5.1 billion (9%). Workplace costs were driven by lost earnings from premature death ($11.2 billion) and reduced compensation/lost employment ($7.9 billion). Health care costs consisted primarily of excess medical and prescription costs ($23.7 billion). Criminal justice costs were largely comprised of correctional facility ($2.3 billion) and police costs ($1.5 billion).
Conclusions. The costs of prescription opioid abuse represent a substantial and growing economic burden for the society. The increasing prevalence of abuse suggests an even greater societal burden in the future.
Introduction
In recent years, the abuse, dependence, and misuse of prescription drugs has become a growing public health concern in the United States. National estimates from the 2007 National Survey on Drug Use and Health (NSDUH) reported that 12.5 million Americans had used prescription pain relievers for nonmedical purposes, up from 11.0 million in 2002 [1]. Of this 12.5 million population, approximately 1.7 million met the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) criteria for abuse or dependence [2]. The 2007 Treatment Episodes Data Set (TEDS) reported that the number of patients admitted to substance abuse treatment facilities due to nonheroin opiate/opioid abuse nearly quadrupled from 23,000 to more than 90,000 from 1999 to 2007 [3]. The Centers for Disease Control and Prevention reported in 2009 that opioid-related poisoning deaths have more than tripled since 1999 [4]. The growing prevalence of prescription opioid abuse, dependence, and misuse (“opioid abuse”) is discussed further in White et al. [5].
As part of the effort to curb the growth of opioid abuse, 34 states have initiated prescription drug monitoring programs (PDMPs) with the purpose of identifying drug abuse and diversion [6]. Furthermore, the Food and Drug Administration (FDA) has recently required certain opioid manufacturers to develop a Risk Evaluation and Mitigation Strategy (REMS) to manage potentially risky prescription drugs and ensure that their benefits outweigh their risks [7]. Despite these initiatives to address opioid abuse, research on the societal economic burden of opioid abuse is limited (e.g., caregiver burden and presenteeism are ignored, as are aspects of the cost to the criminal justice system). Studies by the Office of National Drug Control Policy (ONDCP) and the National Center on Addiction and Substance Abuse report that the overall costs of drug abuse are substantial, but do not quantify the societal burden of opioid abuse specifically [8,9].
In a recent review of the literature, Strassels documented the high costs associated with opioid abuse and cited the estimate by Birnbaum et al. that the societal costs of opioid abuse in 2001 were $11.8 billion; approximately 53% ($6.3 billion, all costs in 2009 USD) of these costs was attributable to lost workplace productivity, 30% ($3.6 billion) to health care, and 17% ($2.0 billion) to criminal justice [10,11]. Focusing specifically on the health care component, White et al. found that during 1998–2002, the excess (i.e., relative to matched controls) annual health care costs per opioid abuse patient in a privately insured population were $17,768, while the diagnosed prevalence of opioid abuse increased from 0.05% to 0.08% during that period [12]. Among Medicaid patients, McAdam-Marx et al. reported costs per abuse patient during 2002–2003 of $18,379 vs $10,952 for controls, and estimated the diagnosed prevalence of opioid abuse in the Medicaid population at 0.87% [13].
The purpose of this study was to evaluate the societal costs associated with prescription opioid abuse in the United States in 2007, drawing on data from a number of different sources. Specifically, this research updates and expands on previous research [11] by including the burden on caregivers (i.e., spouses and dependents of insurance subscribers) as well as additional criminal justice and lost productivity components (e.g., presenteeism costs). The results are disaggregated into three primary categories: health care, criminal justice, and lost workplace productivity.
Methods
Data
This study relied on administrative claims data and on publicly available secondary sources [1,3,5,8,9,14–32] to estimate the societal costs of prescription opioid abuse (see Table 1). All data presented are from the most recent survey or data set for which they are reported, through 2007. For all cost estimates, data are converted to the most recently available year, 2009 USD using the relevant consumer price index (CPI) or hourly compensation index (HCI) (e.g., the CPI for Medical Care was used to adjust health care costs, the HCI was used to adjust wages for work loss costs, and the All Items CPI was used for other cost adjustments) published by the Bureau of Labor Statistics. Administrative claims data were used to estimate excess medical and prescription drug costs as well as excess medically related absenteeism and disability costs for patients diagnosed with opioid abuse. Secondary sources, including academic research, government surveys and publications, and private/nonprofit research, were used in calculating substance abuse treatment, prevention and research costs, criminal justice costs, and lost workplace productivity costs. The manner in which these sources were used in context of the cost calculations is described below (see Cost Analysis section).
Description of data sources
| Data source | Cost component | Description |
| [A] Privately insured employer claims data | Excess medical, drug, medically related absenteeism, and disability costs | Administrative claims for services provided during 2003–2007 from 40 self-insured Fortune 500 companies with locations across the United States |
| [B] Florida Medicaid data | Excess medical, drug, medically related absenteeism, and disability costs | Administrative claims for all Medicaid-eligible beneficiaries for services provided during Q3:2002–Q2:2006 |
| [C] Hadley et al. (2008) [19] | Excess medical and drug costs | Reports nationwide spending per patients for privately insured and uninsured patients |
| [D] Centers for Medicare and Medicaid Services (CMS) (2004) [18] | Excess medical and drug costs | Reports national Medicare spending per capita |
| [E] Kaiser Family Foundation (KFF) (2006) [32] | Excess medical and drug costs | Reports spending per Medicaid beneficiary by state and nationwide, as reported by CMS |
| [F] French et al. (2008) [30] | Substance abuse treatment costs | Reports substance abuse treatment costs |
| [G] National Survey on Drug Use and Health (NSDUH), Substance abuse and Mental Health Services Administration (SAMHSA) (2007) [1] | Ratio of opioid abusers to all drug abusers | Reports the number of Americans reporting substance abuse/dependence by substance |
| [H] Treatment Episodes Data Set (TEDS), SAMHSA (2005–2007) [3] | Substance abuse treatment costs | Reports the number and length of admissions to substance abuse treatment centers |
| [I] Levit et al., SAMHSA (2008) [20] | Substance abuse treatment costs | Reports substance abuse treatment expenditures by source |
| [J] Mark et al., SAMHSA (2007) [21] | Substance abuse treatment costs | Reports the percentage of substance abuse treatment costs attributable to public payers |
| [K] Drug Abuse Warning Network (DAWN), SAMHSA (2007) [17] | Premature death costs | Reports the number of opioid-related deaths and suicides |
| [L] The National Center on Addiction and Substance Abuse at Columbia University (CASA) (2009) [9] | Substance abuse prevention and research costs | Reports substance abuse prevention and research expenditures by source |
| [M] Report on prisoners, Bureau of Justice Statistics (BJS) (2008) [14] | Criminal justice costs | Reports total number of prison inmates by offense and facility type |
| [O] Sourcebook of Criminal Justice Statistics, BJS (2009) [25] | Criminal justice costs | Reports total number of jail inmates by offense |
| [P] Criminal Justice Expenditure and Employment Extracts Program (CJEEP), BJS (2005–2006) [15] | Criminal justice costs | Reports criminal justice expenditures by activity and source |
| [Q] National Forensic Laboratory Information System (NFLIS), Drug Enforcement Agency (DEA) (2008) [24] | Criminal justice costs | Reports the number and type of drug items analyzed in forensic laboratories |
| [R] Uniform Crime Reports, Federal Bureau of Investigation (FBI) (2007) [16] | Criminal justice costs | Reports the number of offenses and arrests and the average value of property lost due to crime |
| [S] Miron JA, Criminal Justice Policy Foundation (2008) [22] | Criminal justice costs | Reports information on police protection and legal and adjudication expenditures |
| [T] Report on the economic costs of drug abuse in the United States, Office of National Drug Control Policy (ONDCP) (2004) [8] | Criminal justice costs, lost wages/employment | Reports the percentage of offenses attributable to drug abuse; reports productivity, losses associated with drug abuse |
| [U] Current Population Survey (CPS), Bureau of Labor Statistics (BLS) (2007) [28] | Workplace costs | Reports population and employment data |
| [V] Hourly Compensation Index, BLS (2007) [29] | Workplace costs | Reports the annual change in average hourly wages in the United States |
| [W] National Vital Statistics Report, Centers for Disease Control and Prevention (CDC) (2006) [23] | Workplace costs | Reports death rates and life expectancy |
| [X] U.S. Census Bureau (2008) [27] | Premature death costs | Reports overall population data |
| [Y] Goetzel et al. (2004) [31] | Presenteeism costs | Reports presenteeism costs for ten common diagnoses relative to health care, medically related absenteeism, and disability costs |
| Data source | Cost component | Description |
| [A] Privately insured employer claims data | Excess medical, drug, medically related absenteeism, and disability costs | Administrative claims for services provided during 2003–2007 from 40 self-insured Fortune 500 companies with locations across the United States |
| [B] Florida Medicaid data | Excess medical, drug, medically related absenteeism, and disability costs | Administrative claims for all Medicaid-eligible beneficiaries for services provided during Q3:2002–Q2:2006 |
| [C] Hadley et al. (2008) [19] | Excess medical and drug costs | Reports nationwide spending per patients for privately insured and uninsured patients |
| [D] Centers for Medicare and Medicaid Services (CMS) (2004) [18] | Excess medical and drug costs | Reports national Medicare spending per capita |
| [E] Kaiser Family Foundation (KFF) (2006) [32] | Excess medical and drug costs | Reports spending per Medicaid beneficiary by state and nationwide, as reported by CMS |
| [F] French et al. (2008) [30] | Substance abuse treatment costs | Reports substance abuse treatment costs |
| [G] National Survey on Drug Use and Health (NSDUH), Substance abuse and Mental Health Services Administration (SAMHSA) (2007) [1] | Ratio of opioid abusers to all drug abusers | Reports the number of Americans reporting substance abuse/dependence by substance |
| [H] Treatment Episodes Data Set (TEDS), SAMHSA (2005–2007) [3] | Substance abuse treatment costs | Reports the number and length of admissions to substance abuse treatment centers |
| [I] Levit et al., SAMHSA (2008) [20] | Substance abuse treatment costs | Reports substance abuse treatment expenditures by source |
| [J] Mark et al., SAMHSA (2007) [21] | Substance abuse treatment costs | Reports the percentage of substance abuse treatment costs attributable to public payers |
| [K] Drug Abuse Warning Network (DAWN), SAMHSA (2007) [17] | Premature death costs | Reports the number of opioid-related deaths and suicides |
| [L] The National Center on Addiction and Substance Abuse at Columbia University (CASA) (2009) [9] | Substance abuse prevention and research costs | Reports substance abuse prevention and research expenditures by source |
| [M] Report on prisoners, Bureau of Justice Statistics (BJS) (2008) [14] | Criminal justice costs | Reports total number of prison inmates by offense and facility type |
| [O] Sourcebook of Criminal Justice Statistics, BJS (2009) [25] | Criminal justice costs | Reports total number of jail inmates by offense |
| [P] Criminal Justice Expenditure and Employment Extracts Program (CJEEP), BJS (2005–2006) [15] | Criminal justice costs | Reports criminal justice expenditures by activity and source |
| [Q] National Forensic Laboratory Information System (NFLIS), Drug Enforcement Agency (DEA) (2008) [24] | Criminal justice costs | Reports the number and type of drug items analyzed in forensic laboratories |
| [R] Uniform Crime Reports, Federal Bureau of Investigation (FBI) (2007) [16] | Criminal justice costs | Reports the number of offenses and arrests and the average value of property lost due to crime |
| [S] Miron JA, Criminal Justice Policy Foundation (2008) [22] | Criminal justice costs | Reports information on police protection and legal and adjudication expenditures |
| [T] Report on the economic costs of drug abuse in the United States, Office of National Drug Control Policy (ONDCP) (2004) [8] | Criminal justice costs, lost wages/employment | Reports the percentage of offenses attributable to drug abuse; reports productivity, losses associated with drug abuse |
| [U] Current Population Survey (CPS), Bureau of Labor Statistics (BLS) (2007) [28] | Workplace costs | Reports population and employment data |
| [V] Hourly Compensation Index, BLS (2007) [29] | Workplace costs | Reports the annual change in average hourly wages in the United States |
| [W] National Vital Statistics Report, Centers for Disease Control and Prevention (CDC) (2006) [23] | Workplace costs | Reports death rates and life expectancy |
| [X] U.S. Census Bureau (2008) [27] | Premature death costs | Reports overall population data |
| [Y] Goetzel et al. (2004) [31] | Presenteeism costs | Reports presenteeism costs for ten common diagnoses relative to health care, medically related absenteeism, and disability costs |
Description of data sources
| Data source | Cost component | Description |
| [A] Privately insured employer claims data | Excess medical, drug, medically related absenteeism, and disability costs | Administrative claims for services provided during 2003–2007 from 40 self-insured Fortune 500 companies with locations across the United States |
| [B] Florida Medicaid data | Excess medical, drug, medically related absenteeism, and disability costs | Administrative claims for all Medicaid-eligible beneficiaries for services provided during Q3:2002–Q2:2006 |
| [C] Hadley et al. (2008) [19] | Excess medical and drug costs | Reports nationwide spending per patients for privately insured and uninsured patients |
| [D] Centers for Medicare and Medicaid Services (CMS) (2004) [18] | Excess medical and drug costs | Reports national Medicare spending per capita |
| [E] Kaiser Family Foundation (KFF) (2006) [32] | Excess medical and drug costs | Reports spending per Medicaid beneficiary by state and nationwide, as reported by CMS |
| [F] French et al. (2008) [30] | Substance abuse treatment costs | Reports substance abuse treatment costs |
| [G] National Survey on Drug Use and Health (NSDUH), Substance abuse and Mental Health Services Administration (SAMHSA) (2007) [1] | Ratio of opioid abusers to all drug abusers | Reports the number of Americans reporting substance abuse/dependence by substance |
| [H] Treatment Episodes Data Set (TEDS), SAMHSA (2005–2007) [3] | Substance abuse treatment costs | Reports the number and length of admissions to substance abuse treatment centers |
| [I] Levit et al., SAMHSA (2008) [20] | Substance abuse treatment costs | Reports substance abuse treatment expenditures by source |
| [J] Mark et al., SAMHSA (2007) [21] | Substance abuse treatment costs | Reports the percentage of substance abuse treatment costs attributable to public payers |
| [K] Drug Abuse Warning Network (DAWN), SAMHSA (2007) [17] | Premature death costs | Reports the number of opioid-related deaths and suicides |
| [L] The National Center on Addiction and Substance Abuse at Columbia University (CASA) (2009) [9] | Substance abuse prevention and research costs | Reports substance abuse prevention and research expenditures by source |
| [M] Report on prisoners, Bureau of Justice Statistics (BJS) (2008) [14] | Criminal justice costs | Reports total number of prison inmates by offense and facility type |
| [O] Sourcebook of Criminal Justice Statistics, BJS (2009) [25] | Criminal justice costs | Reports total number of jail inmates by offense |
| [P] Criminal Justice Expenditure and Employment Extracts Program (CJEEP), BJS (2005–2006) [15] | Criminal justice costs | Reports criminal justice expenditures by activity and source |
| [Q] National Forensic Laboratory Information System (NFLIS), Drug Enforcement Agency (DEA) (2008) [24] | Criminal justice costs | Reports the number and type of drug items analyzed in forensic laboratories |
| [R] Uniform Crime Reports, Federal Bureau of Investigation (FBI) (2007) [16] | Criminal justice costs | Reports the number of offenses and arrests and the average value of property lost due to crime |
| [S] Miron JA, Criminal Justice Policy Foundation (2008) [22] | Criminal justice costs | Reports information on police protection and legal and adjudication expenditures |
| [T] Report on the economic costs of drug abuse in the United States, Office of National Drug Control Policy (ONDCP) (2004) [8] | Criminal justice costs, lost wages/employment | Reports the percentage of offenses attributable to drug abuse; reports productivity, losses associated with drug abuse |
| [U] Current Population Survey (CPS), Bureau of Labor Statistics (BLS) (2007) [28] | Workplace costs | Reports population and employment data |
| [V] Hourly Compensation Index, BLS (2007) [29] | Workplace costs | Reports the annual change in average hourly wages in the United States |
| [W] National Vital Statistics Report, Centers for Disease Control and Prevention (CDC) (2006) [23] | Workplace costs | Reports death rates and life expectancy |
| [X] U.S. Census Bureau (2008) [27] | Premature death costs | Reports overall population data |
| [Y] Goetzel et al. (2004) [31] | Presenteeism costs | Reports presenteeism costs for ten common diagnoses relative to health care, medically related absenteeism, and disability costs |
| Data source | Cost component | Description |
| [A] Privately insured employer claims data | Excess medical, drug, medically related absenteeism, and disability costs | Administrative claims for services provided during 2003–2007 from 40 self-insured Fortune 500 companies with locations across the United States |
| [B] Florida Medicaid data | Excess medical, drug, medically related absenteeism, and disability costs | Administrative claims for all Medicaid-eligible beneficiaries for services provided during Q3:2002–Q2:2006 |
| [C] Hadley et al. (2008) [19] | Excess medical and drug costs | Reports nationwide spending per patients for privately insured and uninsured patients |
| [D] Centers for Medicare and Medicaid Services (CMS) (2004) [18] | Excess medical and drug costs | Reports national Medicare spending per capita |
| [E] Kaiser Family Foundation (KFF) (2006) [32] | Excess medical and drug costs | Reports spending per Medicaid beneficiary by state and nationwide, as reported by CMS |
| [F] French et al. (2008) [30] | Substance abuse treatment costs | Reports substance abuse treatment costs |
| [G] National Survey on Drug Use and Health (NSDUH), Substance abuse and Mental Health Services Administration (SAMHSA) (2007) [1] | Ratio of opioid abusers to all drug abusers | Reports the number of Americans reporting substance abuse/dependence by substance |
| [H] Treatment Episodes Data Set (TEDS), SAMHSA (2005–2007) [3] | Substance abuse treatment costs | Reports the number and length of admissions to substance abuse treatment centers |
| [I] Levit et al., SAMHSA (2008) [20] | Substance abuse treatment costs | Reports substance abuse treatment expenditures by source |
| [J] Mark et al., SAMHSA (2007) [21] | Substance abuse treatment costs | Reports the percentage of substance abuse treatment costs attributable to public payers |
| [K] Drug Abuse Warning Network (DAWN), SAMHSA (2007) [17] | Premature death costs | Reports the number of opioid-related deaths and suicides |
| [L] The National Center on Addiction and Substance Abuse at Columbia University (CASA) (2009) [9] | Substance abuse prevention and research costs | Reports substance abuse prevention and research expenditures by source |
| [M] Report on prisoners, Bureau of Justice Statistics (BJS) (2008) [14] | Criminal justice costs | Reports total number of prison inmates by offense and facility type |
| [O] Sourcebook of Criminal Justice Statistics, BJS (2009) [25] | Criminal justice costs | Reports total number of jail inmates by offense |
| [P] Criminal Justice Expenditure and Employment Extracts Program (CJEEP), BJS (2005–2006) [15] | Criminal justice costs | Reports criminal justice expenditures by activity and source |
| [Q] National Forensic Laboratory Information System (NFLIS), Drug Enforcement Agency (DEA) (2008) [24] | Criminal justice costs | Reports the number and type of drug items analyzed in forensic laboratories |
| [R] Uniform Crime Reports, Federal Bureau of Investigation (FBI) (2007) [16] | Criminal justice costs | Reports the number of offenses and arrests and the average value of property lost due to crime |
| [S] Miron JA, Criminal Justice Policy Foundation (2008) [22] | Criminal justice costs | Reports information on police protection and legal and adjudication expenditures |
| [T] Report on the economic costs of drug abuse in the United States, Office of National Drug Control Policy (ONDCP) (2004) [8] | Criminal justice costs, lost wages/employment | Reports the percentage of offenses attributable to drug abuse; reports productivity, losses associated with drug abuse |
| [U] Current Population Survey (CPS), Bureau of Labor Statistics (BLS) (2007) [28] | Workplace costs | Reports population and employment data |
| [V] Hourly Compensation Index, BLS (2007) [29] | Workplace costs | Reports the annual change in average hourly wages in the United States |
| [W] National Vital Statistics Report, Centers for Disease Control and Prevention (CDC) (2006) [23] | Workplace costs | Reports death rates and life expectancy |
| [X] U.S. Census Bureau (2008) [27] | Premature death costs | Reports overall population data |
| [Y] Goetzel et al. (2004) [31] | Presenteeism costs | Reports presenteeism costs for ten common diagnoses relative to health care, medically related absenteeism, and disability costs |
De-identified administrative claims data used here included a large privately insured population and the Florida Medicaid beneficiaries. The privately insured database covers approximately nine million lives, for services provided during 1999 through 2007, and contains information from 40 self-insured companies, which operate nationwide in a broad array of industries and job classifications. The data include demographic and enrollment information as well as medical, prescription drug, and disability claims for all beneficiaries (i.e., employees, spouses, and dependents). The medical claims contain diagnoses based on codes from the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM), dates, place, type of service, and amounts paid to providers. The drug claims contain information on all prescriptions such as fill date, National Drug Code, days of supply, quantity, and amount paid.
The Florida Medicaid data cover all Medicaid-eligible beneficiaries (over six million lives) between Q3:1997–Q2:2006. The information contained in the Medicaid data is similar to that of the privately insured claims data, although it was not possible to link information at the family level to identify caregivers.
Study Sample: Claims Data
Three study samples were identified and matched to controls: privately insured opioid abuse patients (and a subset of abuse patients who were employed with available work loss data), caregivers of privately insured opioid abuse patients, and Florida Medicaid opioid abuse patients.
Patients were classified as having opioid abuse by identifying those persons with at least one medical claim associated with at least one ICD-9-CM diagnosis for opioid abuse during 2003–2007 (the first such diagnosis was defined as the index date): 304.0 (opioid type dependence), 304.7 (combinations of opioid type dependence with any other drug dependence), 305.5 (opioid abuse), and 965.0 (poisoning by opiates and related narcotics) excluding 965.01 (poisoning by heroin). Opioid abuse patients were required to have at least 6 months of continuous eligibility pre- and postindex date and be 12–64 years old on their index date.
Many definitions of opioid abuse and dependence exist in the literature, with little agreement on which is correct. Note that this study focuses on costs of patients diagnosed with opioid abuse, consistent with White et al., and therefore does not account for undiagnosed opioid abuse patients [12]. Where data on diagnosed abuse was unavailable (which it was for many secondary sources), this study relied on the DSM-IV definition of abuse/dependence, to the extent possible.
Caregivers of privately insured opioid abuse patients (i.e., beneficiaries sharing the same plan as an opioid abuse patient, excluding any with a diagnosis for opioid abuse in their claims history) who had at least one medical or drug claim during 2003–2007 were selected and assigned the same index date as their associated opioid abuse patient. Similar age and eligibility requirements were imposed.
All three samples were matched randomly one-to-one to controls on exact demographic characteristics (age, gender, geographic location, employment status for privately insured, and race for Medicaid). Controls were selected as patients who did not have any diagnoses associated with opioid abuse in their claims history, were not considered a caregiver of an opioid abuse patient, had at least one medical or drug claim during the study period, and met similar age and eligibility requirements. Controls were identified and assigned for all opioid abuse patients. See Table 2 for a description of the demographic profile and Charlson Comorbidity Index of the claims data samples.
Demographics and Charlson Comorbidity Index: Privately Insured and Florida Medicaid Samples, 2003–2007
| Characteristic | Privately insured | Privately insured Caregivers | Florida Medicaid | |||
| Opioid abuse patients (N = 4,474) | Controls (N = 4,474) | Caregivers of opioid abuse patients (N = 5,987) | Controls (N = 5,987) | Opioid abuse patients (N = 4,667) | Controls (N = 4,667) | |
| % | % | % | % | % | % | |
| Demographics | ||||||
| Age (years) | ||||||
| 12–17 | 7.2 | 7.2 | 21.9 | 21.9 | 6.2 | 6.2 |
| 18–34 | 28.1 | 28.1 | 19.6 | 19.6 | 31.7 | 31.7 |
| 35–54 | 48.0 | 48.0 | 46.0 | 46.0 | 52.6 | 52.6 |
| 55–64 | 16.7 | 16.7 | 12.5 | 12.5 | 9.5 | 9.5 |
| Gender | ||||||
| Female | 52.1 | 52.1 | 48.2 | 48.2 | 62.4 | 62.4 |
| Charlson comorbidity index | ||||||
| 0 | 62.6* | 84.0* | 79.4* | 86.8* | 49.0* | 78.3* |
| 1–2 | 22.6* | 12.8* | 14.0* | 11.0* | 29.4* | 15.3* |
| ≥3 | 14.8* | 3.2* | 6.6* | 2.2* | 21.6* | 6.4* |
| Characteristic | Privately insured | Privately insured Caregivers | Florida Medicaid | |||
| Opioid abuse patients (N = 4,474) | Controls (N = 4,474) | Caregivers of opioid abuse patients (N = 5,987) | Controls (N = 5,987) | Opioid abuse patients (N = 4,667) | Controls (N = 4,667) | |
| % | % | % | % | % | % | |
| Demographics | ||||||
| Age (years) | ||||||
| 12–17 | 7.2 | 7.2 | 21.9 | 21.9 | 6.2 | 6.2 |
| 18–34 | 28.1 | 28.1 | 19.6 | 19.6 | 31.7 | 31.7 |
| 35–54 | 48.0 | 48.0 | 46.0 | 46.0 | 52.6 | 52.6 |
| 55–64 | 16.7 | 16.7 | 12.5 | 12.5 | 9.5 | 9.5 |
| Gender | ||||||
| Female | 52.1 | 52.1 | 48.2 | 48.2 | 62.4 | 62.4 |
| Charlson comorbidity index | ||||||
| 0 | 62.6* | 84.0* | 79.4* | 86.8* | 49.0* | 78.3* |
| 1–2 | 22.6* | 12.8* | 14.0* | 11.0* | 29.4* | 15.3* |
| ≥3 | 14.8* | 3.2* | 6.6* | 2.2* | 21.6* | 6.4* |
P < 0.05.
Note: Opioid abuse = opioid abuse, dependence, and misuse.
Demographics and Charlson Comorbidity Index: Privately Insured and Florida Medicaid Samples, 2003–2007
| Characteristic | Privately insured | Privately insured Caregivers | Florida Medicaid | |||
| Opioid abuse patients (N = 4,474) | Controls (N = 4,474) | Caregivers of opioid abuse patients (N = 5,987) | Controls (N = 5,987) | Opioid abuse patients (N = 4,667) | Controls (N = 4,667) | |
| % | % | % | % | % | % | |
| Demographics | ||||||
| Age (years) | ||||||
| 12–17 | 7.2 | 7.2 | 21.9 | 21.9 | 6.2 | 6.2 |
| 18–34 | 28.1 | 28.1 | 19.6 | 19.6 | 31.7 | 31.7 |
| 35–54 | 48.0 | 48.0 | 46.0 | 46.0 | 52.6 | 52.6 |
| 55–64 | 16.7 | 16.7 | 12.5 | 12.5 | 9.5 | 9.5 |
| Gender | ||||||
| Female | 52.1 | 52.1 | 48.2 | 48.2 | 62.4 | 62.4 |
| Charlson comorbidity index | ||||||
| 0 | 62.6* | 84.0* | 79.4* | 86.8* | 49.0* | 78.3* |
| 1–2 | 22.6* | 12.8* | 14.0* | 11.0* | 29.4* | 15.3* |
| ≥3 | 14.8* | 3.2* | 6.6* | 2.2* | 21.6* | 6.4* |
| Characteristic | Privately insured | Privately insured Caregivers | Florida Medicaid | |||
| Opioid abuse patients (N = 4,474) | Controls (N = 4,474) | Caregivers of opioid abuse patients (N = 5,987) | Controls (N = 5,987) | Opioid abuse patients (N = 4,667) | Controls (N = 4,667) | |
| % | % | % | % | % | % | |
| Demographics | ||||||
| Age (years) | ||||||
| 12–17 | 7.2 | 7.2 | 21.9 | 21.9 | 6.2 | 6.2 |
| 18–34 | 28.1 | 28.1 | 19.6 | 19.6 | 31.7 | 31.7 |
| 35–54 | 48.0 | 48.0 | 46.0 | 46.0 | 52.6 | 52.6 |
| 55–64 | 16.7 | 16.7 | 12.5 | 12.5 | 9.5 | 9.5 |
| Gender | ||||||
| Female | 52.1 | 52.1 | 48.2 | 48.2 | 62.4 | 62.4 |
| Charlson comorbidity index | ||||||
| 0 | 62.6* | 84.0* | 79.4* | 86.8* | 49.0* | 78.3* |
| 1–2 | 22.6* | 12.8* | 14.0* | 11.0* | 29.4* | 15.3* |
| ≥3 | 14.8* | 3.2* | 6.6* | 2.2* | 21.6* | 6.4* |
P < 0.05.
Note: Opioid abuse = opioid abuse, dependence, and misuse.
Cost Analysis
Previous studies of the costs of substance abuse provide a useful framework for identifying the major cost categories of health care, criminal justice, and lost workplace productivity [8,9,11]. A prevalence-based estimation approach was used except when estimating productivity losses due to premature death, in which total costs were assigned to the year in which the death occurred. While each category consisted of multiple components that required specific calculations, following previous research, two general approaches were used to estimate costs: 1) a quantity method and (2) an apportionment method [11]. The quantity method multiplies the estimated cost per opioid abuse patient by the relevant number of opioid abuse patients. The apportionment method begins with the overall cost of drug abuse for a particular cost component (taken from a secondary data source) and allocates a cost associated with opioid abuse based on its prevalence relative to overall abuse, as estimated from the number of persons reporting abuse or dependence on prescription opioids in the past 12 months in the 2007 NSDUH. Table 1 provides the data sources for each of the cost analysis methods used for each cost category described below.
Health Care Costs
Health care costs consist of excess medical and drug costs, and substance abuse treatment, prevention, and research costs. Excess medical and drug costs were calculated for both privately insured (Table 1, source [A]) and Florida Medicaid (Table 1, source [B]) opioid abuse patients and privately insured caregivers using the quantity method: excess per-patient costs (costs of patients minus controls derived from actual amounts paid to providers from the claims data) were calculated for all three patient groups, then multiplied by the relevant number of opioid abuse patients (derived from NSDUH {Table 1, source [G]}, who are apportioned to private insurance and Medicaid using TEDS {Table 1, source [H]}), or caregivers (derived as the ratio of caregivers to opioid abuse patients in the privately insured sample {Table 1, source [A]}). To account for differences between Florida Medicaid patients and the national population insured by Medicaid, costs of Florida Medicaid opioid abuse patients were nationally adjusted using the ratio of average spending per Florida Medicaid beneficiary to spending per US Medicaid beneficiary (Table 1, source [E]). Excess medical and drug costs for Medicare and uninsured opioid abuse patients and their caregivers were estimated by applying a national Medicaid-to-Medicare spending ratio (Table 1, sources [D] and [E]) and a privately insured-to-uninsured spending ratio (Table 1, source [C]), respectively.
Treatment, prevention, and research costs were calculated using the apportionment method, by identifying total federal, state, local, and private expenditures on substance abuse treatment, prevention, and research (Table 1, sources [I], [J], and [L]) and multiplying by the proportion associated with opioids (based on the prevalence of opioid abuse relative to overall drug abuse; Table 1, sources [G], [F], and [H]).
Criminal Justice Costs
Calculations for criminal justice costs used the apportionment method to estimate spending associated with opioid abuse on police protection, legal and adjudication, correctional facilities, and property lost due to crime. For each cost component, total spending was identified using data from the Criminal Justice Expenditures and Employment Extract Program (Table 1, source [P]) and the proportion related to opioid abuse was estimated based on the ratio of arrests (for police protection and legal and adjudication components) or incarcerations (for correctional facilities component) attributable to opioid abuse. Arrests or incarcerations attributable to opioid abuse were estimated by first apportioning total arrests or incarcerations for drug law violations and other income-generating and violent crimes (Table 1, sources [M], [O], [R]) to overall drug abuse using published attribution factors (e.g., 100% of drug violations and 30% of burglaries are attributable to drug abuse; Table 1, source [T]), and then apportioning further by multiplying by the ratio of opioid abuse relative to overall drug abuse (Table 1, source [G]) for income-generating and violent crimes, and by the ratio of prescription opioids identified as a percentage of all controlled and uncontrolled substances secured in law enforcement operations (Table 1, source [Q]) for drug law violations.
Lost Workplace Productivity Costs
Lost workplace productivity costs using the human capital approach were calculated using both the quantity and apportionment methods [33]. Similar to excess medical and drug costs, excess medically related absenteeism (i.e., days of lost work due to medical utilization multiplied by daily wage) and disability (i.e., days of lost work due to disability multiplied by daily benefits received) costs were calculated for privately insured employed opioid abuse patients and extrapolated using the quantity method, which multiplies per-patient costs by the number of employees with opioid abuse (Table 1, sources [A], [G] and [H]). Presenteeism costs (i.e., diminished on-the-job productivity) were calculated for employees with opioid abuse and for employed caregivers using a ratio approach used in Goetzel et al. [31] that estimates average presenteeism costs as a percentage of total medical, drug, absenteeism, and disability costs (Table 1, source [Y]).
Lost productivity due to incarceration was estimated by multiplying the per inmate cost of incarceration, in terms of lost wages (calculated as the weighted average of annual expected earnings; Table 1, sources [W] and [U]), by the number of inmates incarcerated for crimes attributable to opioid abuse (described above; Table 1, sources [M], [O], [T], [Q], and [G]). The costs of lost wages/employment were calculated using the apportionment method, by multiplying total lost wages due to lower wages and higher unemployment associated with all drug abuse (Table 1, sources [T] and [V]) by the proportion associated with opioid abuse (Table 1, source [G]).
Finally, consistent with Birnbaum et al. [11], the costs of premature death were calculated by estimating the net present value of lifetime earnings (using a 6% discount rate; Table 1, sources [W], [U]), weighted by age and gender (Table 1, source [X]) and multiplying by the number of deaths related to opioid abuse identified from the Drug Abuse Warning Network (DAWN; Table 1, source [K]).
Results
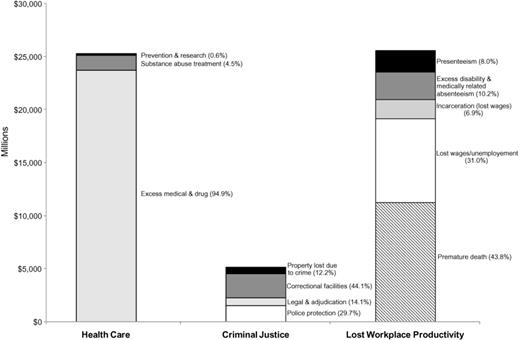
The total societal costs of prescription opioid abuse in 2007 were calculated to be $55.7 billion, of which lost workplace productivity contributed $25.6 billion, health care costs contributed $25.0 billion, and criminal justice costs accounted for the remaining $5.1 billion (Figure 1). Table 3 shows cost estimates for all components of health care, criminal justice, and workplace costs.
Annual societal costs of opioid abuse, dependence, and misuse in the United States: 2007.
Annual societal costs of opioid abuse, dependence, and misuse
| Cost category | Estimation method | Estimated cost (in millions)† ($) | Percentage of total societal costs (%) |
| Health care | |||
| Excess medical and drug (excluding substance abuse treatment)‡ | |||
| Privately insured opioid abuse patients | Quantity | 6,736 | 12.1 |
| Medicaid opioid abuse patients | Quantity | 7,336 | 13.2 |
| Medicare opioid abuse patients | Quantity | 1,010 | 1.8 |
| Uninsured opioid abuse patients | Quantity | 6,861 | 12.3 |
| Privately insured caregivers§ | Quantity | 547 | 1.0 |
| Medicaid caregivers§ | Quantity | 596 | 1.1 |
| Medicare caregivers§ | Quantity | 82 | 0.1 |
| Uninsured caregivers§ | Quantity | 557 | 1.0 |
| All excess medical and drug costs | 23,725 | 42.6 | |
| Substance abuse treatment | |||
| Federal | Quantity | 326 | 0.6 |
| State and local | Quantity | 558 | 1.0 |
| Private | Quantity | 235 | 0.4 |
| All treatment costs | 1,119 | 2.0 | |
| Prevention | |||
| Federal | Apportionment | 52 | 0.1 |
| State and local | Apportionment | 14 | 0.0 |
| Private | Apportionment | 19 | 0.0 |
| All prevention costs | 85 | 0.2 | |
| Research | |||
| Federal | Apportionment | 52 | 0.1 |
| State and local | Apportionment | 2 | 0.0 |
| Private | Apportionment | 16 | 0.0 |
| All research costs | 69 | 0.1 | |
| Total health care costs | 24,998 | 44.9 | |
| Criminal justice | |||
| Police protection | Apportionment | 1,526 | 2.7 |
| Legal and adjudication | Apportionment | 726 | 1.3 |
| Correctional facilities | |||
| Federal | Apportionment | 212 | 0.4 |
| State | Apportionment | 1,430 | 2.6 |
| Local | Apportionment | 623 | 1.1 |
| All correctional facility costs | 2,265 | 4.1 | |
| Property lost due to crime | Apportionment | 625 | 1.1 |
| Total criminal justice costs | 5,142 | 9.2 | |
| Lost workplace productivity | |||
| Premature death | Quantity | 11,218 | 20.1 |
| Lost wages/employment | Apportionment | 7,931 | 14.2 |
| Incarceration (lost wages) | |||
| Federal | Quantity and apportionment | 143 | 0.3 |
| State | Quantity and apportionment | 1,097 | 2.0 |
| Local | Quantity and apportionment | 528 | 0.9 |
| All incarceration costs | 1,768 | 3.2 | |
| Excess medically related absenteeism | |||
| Employees with abuse/dependence | Quantity | 1,171 | 2.1 |
| Employed caregivers | Quantity | 643 | 1.2 |
| All excess medically related absenteeism costs | 1,814 | 3.3 | |
| Excess disability | |||
| Employees with abuse/dependence | Quantity | 727 | 1.3 |
| Employed caregivers | Quantity | 80 | 0.1 |
| All excess disability costs | 807 | 1.4 | |
| Presenteeism | |||
| Employees with abuse/dependence | Quantity | 1,576 | 2.8 |
| Employed caregivers | Quantity | 468 | 0.8 |
| All presenteeism costs | 2,044 | 3.7 | |
| Total workplace costs | 25,582 | 45.9 | |
| Total societal costs (in millions) | 55,721 | 100.0 |
| Cost category | Estimation method | Estimated cost (in millions)† ($) | Percentage of total societal costs (%) |
| Health care | |||
| Excess medical and drug (excluding substance abuse treatment)‡ | |||
| Privately insured opioid abuse patients | Quantity | 6,736 | 12.1 |
| Medicaid opioid abuse patients | Quantity | 7,336 | 13.2 |
| Medicare opioid abuse patients | Quantity | 1,010 | 1.8 |
| Uninsured opioid abuse patients | Quantity | 6,861 | 12.3 |
| Privately insured caregivers§ | Quantity | 547 | 1.0 |
| Medicaid caregivers§ | Quantity | 596 | 1.1 |
| Medicare caregivers§ | Quantity | 82 | 0.1 |
| Uninsured caregivers§ | Quantity | 557 | 1.0 |
| All excess medical and drug costs | 23,725 | 42.6 | |
| Substance abuse treatment | |||
| Federal | Quantity | 326 | 0.6 |
| State and local | Quantity | 558 | 1.0 |
| Private | Quantity | 235 | 0.4 |
| All treatment costs | 1,119 | 2.0 | |
| Prevention | |||
| Federal | Apportionment | 52 | 0.1 |
| State and local | Apportionment | 14 | 0.0 |
| Private | Apportionment | 19 | 0.0 |
| All prevention costs | 85 | 0.2 | |
| Research | |||
| Federal | Apportionment | 52 | 0.1 |
| State and local | Apportionment | 2 | 0.0 |
| Private | Apportionment | 16 | 0.0 |
| All research costs | 69 | 0.1 | |
| Total health care costs | 24,998 | 44.9 | |
| Criminal justice | |||
| Police protection | Apportionment | 1,526 | 2.7 |
| Legal and adjudication | Apportionment | 726 | 1.3 |
| Correctional facilities | |||
| Federal | Apportionment | 212 | 0.4 |
| State | Apportionment | 1,430 | 2.6 |
| Local | Apportionment | 623 | 1.1 |
| All correctional facility costs | 2,265 | 4.1 | |
| Property lost due to crime | Apportionment | 625 | 1.1 |
| Total criminal justice costs | 5,142 | 9.2 | |
| Lost workplace productivity | |||
| Premature death | Quantity | 11,218 | 20.1 |
| Lost wages/employment | Apportionment | 7,931 | 14.2 |
| Incarceration (lost wages) | |||
| Federal | Quantity and apportionment | 143 | 0.3 |
| State | Quantity and apportionment | 1,097 | 2.0 |
| Local | Quantity and apportionment | 528 | 0.9 |
| All incarceration costs | 1,768 | 3.2 | |
| Excess medically related absenteeism | |||
| Employees with abuse/dependence | Quantity | 1,171 | 2.1 |
| Employed caregivers | Quantity | 643 | 1.2 |
| All excess medically related absenteeism costs | 1,814 | 3.3 | |
| Excess disability | |||
| Employees with abuse/dependence | Quantity | 727 | 1.3 |
| Employed caregivers | Quantity | 80 | 0.1 |
| All excess disability costs | 807 | 1.4 | |
| Presenteeism | |||
| Employees with abuse/dependence | Quantity | 1,576 | 2.8 |
| Employed caregivers | Quantity | 468 | 0.8 |
| All presenteeism costs | 2,044 | 3.7 | |
| Total workplace costs | 25,582 | 45.9 | |
| Total societal costs (in millions) | 55,721 | 100.0 |
All costs are reported in 2009 USD.
Estimates of excess health care costs include patients exhibiting clinical abuse/dependence and do not include patients engaging only in nonmedical use.
Caregivers are defined as dependents or spouses of patients with abuse or dependence, but who do not meet criteria for abuse or dependence themselves.
Annual societal costs of opioid abuse, dependence, and misuse
| Cost category | Estimation method | Estimated cost (in millions)† ($) | Percentage of total societal costs (%) |
| Health care | |||
| Excess medical and drug (excluding substance abuse treatment)‡ | |||
| Privately insured opioid abuse patients | Quantity | 6,736 | 12.1 |
| Medicaid opioid abuse patients | Quantity | 7,336 | 13.2 |
| Medicare opioid abuse patients | Quantity | 1,010 | 1.8 |
| Uninsured opioid abuse patients | Quantity | 6,861 | 12.3 |
| Privately insured caregivers§ | Quantity | 547 | 1.0 |
| Medicaid caregivers§ | Quantity | 596 | 1.1 |
| Medicare caregivers§ | Quantity | 82 | 0.1 |
| Uninsured caregivers§ | Quantity | 557 | 1.0 |
| All excess medical and drug costs | 23,725 | 42.6 | |
| Substance abuse treatment | |||
| Federal | Quantity | 326 | 0.6 |
| State and local | Quantity | 558 | 1.0 |
| Private | Quantity | 235 | 0.4 |
| All treatment costs | 1,119 | 2.0 | |
| Prevention | |||
| Federal | Apportionment | 52 | 0.1 |
| State and local | Apportionment | 14 | 0.0 |
| Private | Apportionment | 19 | 0.0 |
| All prevention costs | 85 | 0.2 | |
| Research | |||
| Federal | Apportionment | 52 | 0.1 |
| State and local | Apportionment | 2 | 0.0 |
| Private | Apportionment | 16 | 0.0 |
| All research costs | 69 | 0.1 | |
| Total health care costs | 24,998 | 44.9 | |
| Criminal justice | |||
| Police protection | Apportionment | 1,526 | 2.7 |
| Legal and adjudication | Apportionment | 726 | 1.3 |
| Correctional facilities | |||
| Federal | Apportionment | 212 | 0.4 |
| State | Apportionment | 1,430 | 2.6 |
| Local | Apportionment | 623 | 1.1 |
| All correctional facility costs | 2,265 | 4.1 | |
| Property lost due to crime | Apportionment | 625 | 1.1 |
| Total criminal justice costs | 5,142 | 9.2 | |
| Lost workplace productivity | |||
| Premature death | Quantity | 11,218 | 20.1 |
| Lost wages/employment | Apportionment | 7,931 | 14.2 |
| Incarceration (lost wages) | |||
| Federal | Quantity and apportionment | 143 | 0.3 |
| State | Quantity and apportionment | 1,097 | 2.0 |
| Local | Quantity and apportionment | 528 | 0.9 |
| All incarceration costs | 1,768 | 3.2 | |
| Excess medically related absenteeism | |||
| Employees with abuse/dependence | Quantity | 1,171 | 2.1 |
| Employed caregivers | Quantity | 643 | 1.2 |
| All excess medically related absenteeism costs | 1,814 | 3.3 | |
| Excess disability | |||
| Employees with abuse/dependence | Quantity | 727 | 1.3 |
| Employed caregivers | Quantity | 80 | 0.1 |
| All excess disability costs | 807 | 1.4 | |
| Presenteeism | |||
| Employees with abuse/dependence | Quantity | 1,576 | 2.8 |
| Employed caregivers | Quantity | 468 | 0.8 |
| All presenteeism costs | 2,044 | 3.7 | |
| Total workplace costs | 25,582 | 45.9 | |
| Total societal costs (in millions) | 55,721 | 100.0 |
| Cost category | Estimation method | Estimated cost (in millions)† ($) | Percentage of total societal costs (%) |
| Health care | |||
| Excess medical and drug (excluding substance abuse treatment)‡ | |||
| Privately insured opioid abuse patients | Quantity | 6,736 | 12.1 |
| Medicaid opioid abuse patients | Quantity | 7,336 | 13.2 |
| Medicare opioid abuse patients | Quantity | 1,010 | 1.8 |
| Uninsured opioid abuse patients | Quantity | 6,861 | 12.3 |
| Privately insured caregivers§ | Quantity | 547 | 1.0 |
| Medicaid caregivers§ | Quantity | 596 | 1.1 |
| Medicare caregivers§ | Quantity | 82 | 0.1 |
| Uninsured caregivers§ | Quantity | 557 | 1.0 |
| All excess medical and drug costs | 23,725 | 42.6 | |
| Substance abuse treatment | |||
| Federal | Quantity | 326 | 0.6 |
| State and local | Quantity | 558 | 1.0 |
| Private | Quantity | 235 | 0.4 |
| All treatment costs | 1,119 | 2.0 | |
| Prevention | |||
| Federal | Apportionment | 52 | 0.1 |
| State and local | Apportionment | 14 | 0.0 |
| Private | Apportionment | 19 | 0.0 |
| All prevention costs | 85 | 0.2 | |
| Research | |||
| Federal | Apportionment | 52 | 0.1 |
| State and local | Apportionment | 2 | 0.0 |
| Private | Apportionment | 16 | 0.0 |
| All research costs | 69 | 0.1 | |
| Total health care costs | 24,998 | 44.9 | |
| Criminal justice | |||
| Police protection | Apportionment | 1,526 | 2.7 |
| Legal and adjudication | Apportionment | 726 | 1.3 |
| Correctional facilities | |||
| Federal | Apportionment | 212 | 0.4 |
| State | Apportionment | 1,430 | 2.6 |
| Local | Apportionment | 623 | 1.1 |
| All correctional facility costs | 2,265 | 4.1 | |
| Property lost due to crime | Apportionment | 625 | 1.1 |
| Total criminal justice costs | 5,142 | 9.2 | |
| Lost workplace productivity | |||
| Premature death | Quantity | 11,218 | 20.1 |
| Lost wages/employment | Apportionment | 7,931 | 14.2 |
| Incarceration (lost wages) | |||
| Federal | Quantity and apportionment | 143 | 0.3 |
| State | Quantity and apportionment | 1,097 | 2.0 |
| Local | Quantity and apportionment | 528 | 0.9 |
| All incarceration costs | 1,768 | 3.2 | |
| Excess medically related absenteeism | |||
| Employees with abuse/dependence | Quantity | 1,171 | 2.1 |
| Employed caregivers | Quantity | 643 | 1.2 |
| All excess medically related absenteeism costs | 1,814 | 3.3 | |
| Excess disability | |||
| Employees with abuse/dependence | Quantity | 727 | 1.3 |
| Employed caregivers | Quantity | 80 | 0.1 |
| All excess disability costs | 807 | 1.4 | |
| Presenteeism | |||
| Employees with abuse/dependence | Quantity | 1,576 | 2.8 |
| Employed caregivers | Quantity | 468 | 0.8 |
| All presenteeism costs | 2,044 | 3.7 | |
| Total workplace costs | 25,582 | 45.9 | |
| Total societal costs (in millions) | 55,721 | 100.0 |
All costs are reported in 2009 USD.
Estimates of excess health care costs include patients exhibiting clinical abuse/dependence and do not include patients engaging only in nonmedical use.
Caregivers are defined as dependents or spouses of patients with abuse or dependence, but who do not meet criteria for abuse or dependence themselves.
Lost Workplace Productivity Costs
Lost workplace productivity costs contributed the largest share of total societal costs with approximately $25.6 billion, or 45.9%, of total societal costs. Of the workplace costs, the cost of premature death was the largest component, accounting for $11.2 billion (43.8%), and lost wages/employment and presenteeism were the next two costliest components, contributing $7.9 billion (31.0%) and $2.0 billion (8.0%), respectively. Excess medically related absenteeism and incarceration costs accounted for comparable amounts at $1.8 billion (7.1%) and $1.8 billion (6.9%), respectively, while excess disability costs accounted for only $807 million (3.2%). Employees with opioid abuse accounted for 64.5% and 90.1% of excess medically related absenteeism and disability costs, while caregivers contributed the remaining 35.5% and 9.9%, respectively.
Health Care Costs
Health care costs accounted for approximately $25.0 billion, or 44.9%, of total societal costs, of which excess medical and drug costs were the main drivers, contributing $23.7 billion (94.9%). Opioid abuse patients accounted for over 92% of excess medical and drug costs, with their caregivers accounting for the remainder. Medicaid patients and caregivers combined contributed approximately one-third of total excess medical and drug costs, privately insured and uninsured patients and caregivers contributed slightly less than one-third each, and Medicare patients and caregivers accounted for only 4.6%.
Of total health care costs, substance abuse treatment, prevention, and research all contributed a substantially smaller amount, accounting for costs of $1.1 billion (4.5%), $85 million (0.3%), and $69 million (0.3%), respectively. Substance abuse research and prevention expenditures together contributed merely 0.3% of the total societal costs, with the majority of funding provided by federal sources. Treatment, in contrast, contributed a slightly larger share of the total, 2.0%, and consisted primarily of state and local expenditures, followed by federal and private funding.
Criminal Justice Costs
Criminal justice costs contributed approximately $5.1 billion, or 9.2% of the total societal costs, of which correctional facilities accounted for the largest share with $2.3 billion (44.1%). Of these correctional facility costs, nearly two-thirds were incurred at the state level. Of total criminal justice costs, police protection contributed $1.5 billion (29.7%), legal and adjudication costs accounted for $726 million (14.1%), and the costs associated with property lost due to crime accounted for $625 million (12.2%).
Discussion
The results of this analysis document that the growing problem of prescription opioid abuse places a substantial economic burden on society, specifically in the realms of health care, criminal justice, and lost workplace productivity.
Implications
These findings provide further evidence that prescription opioid abuse is an increasing and substantial burden on society that needs to be addressed in a comprehensive manner. As discussed above, the impact of opioid abuse not only affects the health outcomes and costs of the US population ($25.0 billion), but also imposes a large economic burden on the workplace ($25.6 billion), the justice system ($5.1 billion), and society as a whole ($55.7 billion). Although differences in data and methods preclude exact comparison with previous societal estimates [11], it is clear that the costs of opioid abuse have increased substantially due to changes in the prevalence of opioid abuse and associated costs. Key changes include, for example, increases from 2001 to 2007 (compared with Birnbaum et al. [11]) in the prevalence of opioid abuse (approximately 13%), the excess cost per opioid abuse patient (47% after adjusting for inflation), the cost of substance abuse treatment (up to 48%), the proportion of substance abuse admissions attributable to opioids (138%), and total police and legal expenditures (16% and 10%, respectively).
Reducing the substantial economic burden of prescription opioid abuse will require sustained efforts from academic researchers, industry, health care providers, and government to implement appropriate actions. A number of initiatives to reduce the prevalence of opioid abuse are already underway. For example, government initiatives such as the National All Schedules Prescription Electronic Reporting Act (NASPER) have allocated funding for the creation and enhancement of state PDMPs [34]. The FDA now requires the preparation of a REMS for certain prescription opioid manufacturers. Industry has begun to manufacture abuse-deterrent opioid formulations, and clinical initiatives have included the publication and adoption of “universal precautions” for pain management as well as the development of models to better identify patients at risk of opioid abuse [35–37].
In particular, the difference between overall societal costs and the current level of spending on research and prevention is quite substantial, with such expenditures together accounting for less than 1% of total societal costs. Thus, increased funding of research and prevention programs may present an opportunity for new efforts to combat the escalating problem of prescription opioid abuse. The benefits of investing more resources into these two components could be considerable, since adequate prevention and research programs could later result in reductions in excess medical and drug costs (estimated at $23.7 billion), treatment costs ($1.1 billion), and other cost components previously discussed, such as criminal justice ($5.1 billion) and lost workplace productivity ($25.6 billion). The adoption of PDMPs to identify patients at risk of abuse in many states is a step in the right direction, but 16 states still have yet to implement PDMPs, including nine which have not even passed legislation mandating their creation [6].
Limitations
Despite the evident growth in prevalence and treatment admissions associated with opioid abuse, quantifying the growth in societal costs is not straightforward; recent improvements in the analytic approaches and changes in data collection methodology make overall comparison with previous results difficult [11]. For example, this study calculates cost categories not previously estimated, such as those of caregivers, prevention and research, property lost due to crime, excess medically related absenteeism, disability, and presenteeism. To further confound the comparison, the current study includes costs associated with opioid dependence as well as abuse (which was the only aspect of abuse considered previously), and criminal justice costs here include those associated with violent crime. Some secondary data sources, such as DAWN and NSDUH, also have updated their methodologies. To the extent that comparisons can be made, claims data estimates are consistent with prior research and suggest an increase in the costs of abuse, even after controlling for inflation.
There are several other limitations to this study. Florida Medicaid figures are not representative of the national Medicaid population, as Florida spends only $4,487 per Medicaid enrollee, ranking it 43rd and below the national average of $5,163 [32]. However, as noted, these data were adjusted to the US Medicaid population based on a per enrollee spending ratio.
This study is also limited by the variability among the distinct secondary data sets. However, adjusting the opioid abuse-related allocation of a specific component allowed for increased compatibility among different sources. For example, when using the apportionment method to estimate substance abuse prevention costs associated with prescription opioids, total prevention costs (which include spending for illicit and prescription drug, alcohol, and tobacco abuse prevention) were apportioned based on the ratio of NSDUH-reported abuse of prescription opioids to abuse of illicit drugs, alcohol, or tobacco, whereas lost wages/employment costs (which include costs due to illicit drug abuse) were apportioned based on the ratio of NSDUH-reported abuse of prescription opioids to abuse of illicit drugs only. Notwithstanding this, the different definitions and concepts of opioid abuse make comparisons across data sets problematic. To the authors' knowledge, this is the first attempt to integrate the different data sets in one analysis.
In addition to the difficulty in addressing variability between data sets, the secondary sources used have their own limitations. Data from DAWN used to calculate the number of premature deaths associated with opioid abuse represent drug-related deaths in selected metropolitan areas and states only, and may not be representative of drug-related death patterns in areas not reported. To the authors' knowledge, DAWN data provide the best available estimate of drug-related deaths in the United States. Attribution factors from ONDCP used to apportion arrests and incarcerations due to drug abuse were developed prior to 2007, and therefore may not accurately represent the proportion of arrests and incarcerations attributable to drug abuse. However, criminal justice costs may be underestimated because the overall number of reported drug abusers has grown at a much higher rate than the overall number of arrests since the development of the attribution factors. Conversely, in this case, the apportionment method used may lead to overestimation because prescription opioid abuse may not be associated with the same likelihood of arrest as abuse of other drugs. Additionally, presenteeism costs were estimated using a ratio of average presenteeism costs relative to overall medical, drug, absenteeism, and disability costs reported in Goetzel et al. for the 10 most common conditions examined (e.g., allergies, cancer, depression/mental illness) [31]. Because opioid abuse specific estimates were not available, it was assumed that presenteeism costs for employees with opioid abuse followed the same ratio.
As noted above, there are various issues in defining opioid abuse. For example, ICD-9-CM codes do not allow for differentiation between prescription opioid abuse and heroin abuse, and therefore, this study likely included both types of patients. Where possible, heroin abuse was separated from prescription opioid abuse in cost analyses using secondary data sources. This study estimates costs using two general definitions of abuse. First, per-patient excess medical and drug costs were calculated using a diagnosis-based definition. This approach captured patients with abuse, dependence, and misuse (e.g., poisoning). Opioid abuse may be underdiagnosed due, in part, to the associated stigma [38], and therefore the patient population used to calculate excess costs may not be representative of the cost profile of undiagnosed patients with opioid abuse. Second, the number of opioid abuse patients used to carry out the quantity and apportionment methods was limited to those reported by NSDUH as meeting the DSM-IV criteria for abuse or dependence (1.7 million), similar to an ICD-9-CM diagnostic approach to abuse. The absence of cost information for the approximately 12.5 million nonmedical users of prescription drugs [1] and their caregivers in the United States means that this study likely understates both the excess health care and total societal costs. It is also important to mention that this study does not attempt to address causality. While the societal costs refer to those costs associated with opioids abusers, they may not be directly attributable to the opioid abuse. For example, health care costs include costs of comorbidities that are unrelated to opioid abuse per se. While point estimates of the various measures of societal cost have not been presented here, the authors believe the estimates understate the true economic burden of prescription opioid abuse, dependence and misuse, and thus these estimates are conservative.
To better understand how various assumptions impacted the total societal cost estimate, sensitivity analyses were conducted. The primary driver of societal costs was the number of opioid abusers, which is used to multiply costs per patient in all cost components that use the quantity method. Changing the number of opioid abusers by ±25% impacts the total societal cost estimate by $10 billion ($45.7–65.7 billion). This finding suggests that the increasing prevalence of opioid abuse may be driving increases in societal costs. Another key assumption is the discount rate used in the calculation of the costs of premature death. For example, if the discount rate were decreased to 3%, the societal cost estimate would increase from $55.7 billion to $61.2 billion. While current market conditions may suggest that a lower rate could be more appropriate, 6% is consistent with past research [11] and results in a more conservative cost estimate. A systematic analysis that varied other major assumptions for each cost component by 25% (all else equal) found that no other individual assumption resulted in a change of more than $2 billion in the overall societal cost estimate.
Future research should attempt to assess other components of societal costs that are directly linked to or caused by prescription opioid abuse not considered here (e.g., automobile accidents, insurance fraud, workers compensation) as well as improve understanding of the relationship between opioid abuse and associated comorbidities (e.g., by studying whether mental illness predates a diagnosis of opioid abuse or vice versa). It would also be informative to analyze the costs of undertreating pain, which can result from practitioners' concerns about addiction and abuse [39].
Further efforts to separately categorize prescription and nonprescription opioid abuse would allow researchers to better understand illicit opioid use as well as identify possible sources of distribution. Lastly, it would be useful to improve the ability to identify patients at risk of opioid abuse using data similar to that available to PDMPs and third-party payers, similar to the prototype approach developed by White et al. but using national data [37]. Such an approach could aid in the development of national initiatives and research studies toward the prevention of opioid abuse.
As this study has shown, prescription opioid abuse concerns far more than those individuals directly affected by the condition. It is associated with a myriad of societal problems related to productivity losses and increasing criminal and legal justice costs that are rapidly becoming a major public health and economic concern. A multifaceted, coordinated response involving physicians, health care professionals, researchers (including the pharmaceutical industry), and the government is likely required to make substantial progress on this serious issue.
Role of Funding Source
Funding for this study was provided by King Pharmaceuticals, Inc.
Contributors
Howard Birnbaum, Alan White, and Carl Roland designed and wrote the protocol. Matt Schiller and Tracy Waldman conducted the secondary data collection and with Jody Cleveland undertook the statistical analysis. All authors contributed to the writing of the manuscript and have approved the final manuscript.
Conflict of Interest
Carl Roland and Jody Cleveland are employees of King Pharmaceuticals, Inc. Howard Birnbaum, Alan White, Matt Schiller, and Tracy Waldman are employees of Analysis Group, Inc., who received support for this research from King Pharmaceuticals, Inc.
Acknowledgements
The authors would like to acknowledge Diego Barido, BA, Analysis Group, Inc., for his research support.

{kind=link}