





Summary
This article describes the process by which ‘flat feet’ became a well-recognised medical diagnosis and eventually came to be seen as an important indicator of national health during early twentieth-century America. I argue that orthopaedic surgeons—a relatively new medical specialty at the time—took a leading role in this process. During the First World War, they standardised diagnostic measures for flat feet as a way to delineate ‘fit’ from ‘unfit’ draftees, rejecting the latter from military service (a practice that persisted for the remainder of the century). But instead of sending the ‘unfit’ home, orthopaedic surgeons believed that they could rehabilitate rejected draftees using techniques such as stretching and strengthening exercises in order to make the flatfooted into foot-fit men. After the war, these same surgeons applied their theory of rehabilitation to the industrial workplace, where they supplanted physiologists as the new experts on bodily efficiency, a move that would eventually bring about the science of body mechanics and ergonomics. Finally, I argue that wartime orthopaedics serves as an important example of social medicine in practice during the early twentieth century. Orthopaedic surgeons contended that physical disability was as much of a threat to national health as germs and believed that debilitating conditions such as flat feet should be prevented and cured for the general betterment of American society.
Almost as soon as the last shot was fired in Europe, bringing an end to the First World War in November 1918, the United States Public Health Service (USPHS) began an educational campaign that equated American national power with physical, bodily strength. In its 1919 ‘Keep Well Series’, the USPHS wrote with great alarm that military medical exams showed that about one-third of American draftees were physically ‘unfit’, suffering from one kind of defect or another. One of the most common defects was ‘flat feet’, a term applied to men whose longitudinal arches—the inner arch of the foot—were fallen, almost flat on the ground. 1 A later study in 1920 published by the US Army Surgeon General's Office estimated that roughly 10 per cent of those called for service suffered from flat feet, making the condition one of the most common physical debilities that kept American men out of the Army. 2 While the study indicated that almost as many American men were exempted from duty because of reasons ranging from genital varicosities to malnutrition, flat feet captured more attention from the US Army than any of the other maladies would. 3
The fact that the US Army rejected almost one-tenth of its military volunteers and draftees because of ‘deformed’ feet is even more striking when these figures are compared to those of the armed forces in Great Britain. According to historian Jay Winter, while ‘severe’ flat foot demoted a British military conscript to a ‘C-III’ status (A-I was the highest physical score possible, and D-IV the lowest), the condition did not warrant military rejection; instead it indicated that the recruit was fit for military work, but only at home. 4 Additionally, medical historian Joel Howell has shown that British medical officers during the Great War worried more about the soldier's heart than his feet. 5
Why did flat feet become a point of fixation for the US government, the Army, and so many other Americans during and after the First World War? 6 How did it become defined as an incapacitating disability that threatened not only America's military power but also the strength of civil society as a whole? How, moreover, was it possible for a nation to devote so much time and money to the eradication of flat feet when, as latecomers to the war, US military authorities knew that the country would face more damaging injuries such as trench foot, peripheral nerve paralysis, and amputations that left returning soldiers with no feet at all?
This essay argues that part of the answer to these questions lies in orthopaedic surgery, a medical specialty that won autonomy over its own divisional unit in the US Army's Medical Department during the Great War. Orthopaedists succeeded in drawing nationwide attention to flat feet because they defined it as a social ill instead of as a circumscribed medical problem—as a threat to America's military, industrial and economic strength, rather than as a danger to individual bodily health. 7 They characterised flat feet as a preventable medical problem, one that could be avoided with a dose of public education along with repeated bouts of daily exercise. Unlike other branches of surgery—such as obstetrics, neurosurgery and plastic surgery—which used the scalpel and other specialised technologies to shape professional identity, orthopaedists adhered to the most conservative form of surgery. 8 Their professional identity was shaped, in other words, by an ideological commitment to non-invasive physical medicine—such as stretching, strengthening exercises and bandaging—and to the belief that this type of physical medicine would lead to the betterment of society.
Ultimately, by taking flat feet out of the domain of acute medicine—where braces, hardware and radical operations were used—and putting it under the rubric of preventative and sub-acute rehabilitative care, wartime orthopaedic surgeons engaged in a form of social medicine. To be sure, military orthopaedists were not political radicals or revolutionaries like the more better known advocates of social medicine during the nineteenth century; orthopaedists worked within the system of industrial capitalism, fixing the injurious results from modern warfare and the workplace rather than questioning why such disabilities occurred in the first place. 9 Nevertheless, their belief that flat feet was a debilitating condition that should be cured for the general betterment of society places them among the ranks of health care professionals who wanted to bring about social change rather than mere medical specialism and clinically-oriented therapeutic cures. 10
Pre-War Concerns
Well before the First World War, the soldier's foot had been a topic of discussion among a wide array of military strategists throughout the Western hemisphere. In one military classic from 1901, The Art of Marching , George Armand Furse contended that ‘mobility’ was the first requisite of the soldier and that marching was the most important factor to winning wars, often more important than the ‘art of fighting’. Without healthy and pain-free feet, a ‘foot soldier’ could not fulfil the duty implied in his title. Armies throughout the modern Western world followed Napoleon's mandate that ‘getting there first with the most men’ assured victory. 11
In the American context, however, wartime foot problems received attention only on a case-by-case basis before the First World War. While it is reputed that President Abraham Lincoln recommended his own personal podiatrist, Isachar Zacharie, for the Union Army's ‘Commission of Chiropodist General of the United States’, such a department never materialised. 12 Instead, as historian Mary C. Gillette points out, neither the Union nor Confederate armies had standardised physical exams, diagnoses or methods of prescription that uniformly addressed the health of a soldier's foot. Medical examinations of Civil War recruits varied from state to state, and because of the pressing need for more and more men on the front lines, military physicians became lax in their examinations, leading to armies of ‘consumptives, asthmatics, one-eyed and one-armed men’. 13 The US military did not push for standardised medical exams until after the Spanish-American War when President Theodore Roosevelt, a long time advocate of physical fitness and the outdoor life, insisted on mandatory yearly physical exams of all field officers in order to control the prevalence of ‘obesity’ among middle-aged officers. 14
Along with the advent of uniform physical examinations in the wake of the Spanish-American War, the US Army also became interested in standardising military footwear. Following in line with the general trend in civil society towards standardisation in the manufacturing of shoes and the measurement of feet, Surgeon General George H. Torney commissioned an Army Shoe Board in 1908, making the soldier's foot a priority in military research and investigation. 15 Major Edward L. Munson of Fort Leavenworth, Kansas, a surgeon with a particular interest in orthopaedics and ill-fitting shoes, led the four-year investigation, examining over 2,000 soldiers. Munson published the results of his investigation in 1912, and concluded that more than half of the Army's soldiers wore shoes that were too small for them. 16 In order to solve the Army's footwear problem, Munson devised his own military boot using a wider and thicker shoe mold, known as a ‘last’. With his study, Munson not only introduced the first standardised Army-issued boot, but he also argued that his method of measuring the foot would prove to be a strategic military benefit. By shifting control over footwear from the individual soldier (who before the 1910s relied on local cobblers for shoes) to commanding officers, Munson empowered infantry leaders with objective measures that undercut subjective complaints about sore feet, a grievance that often kept fighting men from marching. 17
To further persuade the US Army of his views, Munson's bolstered his argument by using the research of other well-known orthopaedic surgeons who, during the late nineteenth century, began to voice concern about ‘shoemaker-made feet’. 18 Royal Whitman, chief of orthopaedic surgery at the Hospital for the Ruptured and Crippled (now the Hospital for Special Surgery) in New York City, led the charge, arguing that the prevalence of so-called ‘foot disability’ was a problem created by shoe manufacturers who preyed on the ignorance of their customers. 19 Not appreciating the anatomy of the foot, shoe manufacturers, according to Whitman, followed the whimsy of fashion rather than foot function. Whitman and his colleagues railed against high heels worn by women, and the narrow, ‘toothpick shoes’ worn by men. Revealing Whitman's influence on his thinking, Munson argued that it was ‘rare to find in civil life a shoe that even approaches the normal foot in shape and contour’; shoes were, rather, erroneously constructed by taste, styles and ‘sightliness’. 20
The campaign that turn-of-the-century orthopaedic surgeons waged against shoe manufacturers was, in many ways, the logical outgrowth of the Victorian clothing reform movement in which certain health advocates criticised fashionable clothing, such as corsets and long skirts, as being dangerous to a person's bodily functions and overall well being. 21 As a result of this clothing reform, posture in the post-Victorian era became something that required muscular control rather than properly restrictive outerwear. 22 In this muscularly aware context, orthopaedic surgeons focused on the structure of the feet as the basis—the foundation, even—for maintaining good posture. Taking their cue from Victorian clothing reformers, orthopaedists such as Whitman argued the most fashionable high-heeled and narrow-toed shoes created serious foot deformities.
While other orthopaedic surgeons and foot specialists argued that patients with flat feet needed to be surgically treated or fitted with braces, Whitman argued the opposite, contending that flat feet was a problem of muscle weakness that could be overcome with appropriate medical treatment and exercise. Whitman strongly opposed those physicians who believed flat feet to be an inherited condition, arguing instead that it was a structural deformity that could be ‘actively treated and permanently cured’. 23
Making his campaign against toothpick shoes public, Whitman emerged as the single most important voice on the matter of flat feet for the US Army, not necessarily because he had the best or truest description of the condition, but because his theories on its aetiology and treatment appealed to the military. In the final version of The Soldier's Foot and the Military Shoe , for instance, Major Munson depended on Whitman's description, aetiology and treatment of flat foot. Munson even replicated the diagrams that Whitman used to explain flat feet. Because Munson's book became a medical handbook issued to every military medical officer from 1912 to the First World War, the Army served as a kind of clearing house for Whitman's ideas and theories of treatment.
With his specialised theories of the foot, Whitman made flat feet into a fully conceptualised disability that threatened the very integrity of the nation's military power and strength. Although he painted a grim picture of flat feet, he simultaneously held out the hope that the US Army, and indeed the nation as a whole, could rid itself of the condition with enough orthopaedic awareness and persistence. Long seen as the dredges of society, line soldiers who came to the Army with unseemly foot deformities would be accepted into the military ranks in the faith not only that such a deformity could be cured, but also that the military would do its part in improving the health, strength and outward appearance of its nation's citizens.
Standardising Foot Exams during the War
As a result of Whitman's popularity, more and more orthopaedic surgeons during the first two decades of the twentieth century found it acceptable to have a specialised interest in the human foot. Foot specialisation became even more respectable when the Great War commenced. Initial reports coming from Germany and France in 1914 indicated that flat feet greatly hindered military efficiency. By the winter of 1914, however, European military concerns about flat feet ceased as the demands of trench warfare required more static manpower—men sitting with rifles in water-laden trench dug-outs—than mobile foot soldiers marching to conquer new territory. With enemy forces separated by a mere five to ten yards along certain parts of the Western front, soldiers fought the war by leaping from the trenches and heading directly into enemy fire.
Orthopaedic surgeons in the United States, nevertheless, took hold of the warnings about flat feet coming from Europe and, by 1915, used the Continent as evidence for the creation of an ‘Orthopedic War Preparedness Committee’, a group that would inform both the American Orthopedic Association (AOA) and the American Medical Association of the growing need for military orthopaedics. Although under President Woodrow Wilson the US remained neutral for the first three years of the Great War, Joel E. Goldthwait—president of the AOA and the preparedness committee—wrote in 1915 that the United States ‘would ultimately assume some part in the struggle’. 24 For most of the war, then, American orthopaedists made recommendations based on a unique perspective of the war, from a place removed from the fighting. They discussed and analysed the medical needs of soldiers with their European colleagues from the safety of their own homes, never having to see soldiers suffering from war-inflicted injuries first hand. For this reason, US orthopaedic surgeons had the luxury of time and security to think more about prevention of injury than about actual war-torn bodies.
From the very beginning, Goldthwait, an 1890 graduate of Harvard Medical School and a prominent Massachusetts orthopaedist, recruited several of his closest Boston colleagues to help persuade the US Army, and more specifically the US Medical Department, that orthopaedic surgery was essential to military preparedness. Goldthwait first appointed Doctors Robert Osgood and Nathaniel Allison—both of whom had left Boston in 1914 to volunteer their services to Dr Robert Jones, the pioneering innovator in Britain—since they had first-hand wartime orthopaedic experience. Goldthwait also relied on the advice of his Massachusetts General Hospital colleague, Elliot Brackett, who would become chief of the Orthopedics Section of the US Medical Corps during the First World War, as well as from Robert Williamson Lovett, another well-known Boston surgeon who took charge of military orthopaedic education at Harvard for the duration of the war.
Although the Boston group of orthopaedic surgeons based their arguments of orthopaedic necessity on figures coming in from Europe, they also relied on their own pre-war experiences with flat feet. Both Lovett and Osgood, for instance, had performed flat feet research on nurses at the Massachusetts General Hospital and the Boston City Hospital. 25 In 1911, Osgood argued that since the ligaments of the foot were ‘not wholly elastic’ and would ‘stretch if subject to a constant strain’, the ‘ muscular anatomy of the foot’ was the single ‘most important factor in maintaining proper weight-bearing lines’. 26 Coming to the conclusion that muscles mattered most, Osgood insisted that the best antidote to the prevalence of flat foot was preventive medicine—a programme of education on the anatomy of the foot, proper shoe wear and instruction in exercises for the feet.
To the Boston orthopaedic surgeons who helped outline the ‘orthopedic preparedness’ report for the Army Surgeon General in 1916, what applied to the working feet of hospital nurses also applied to military soldiers. According to such assessments, orthopaedic surgeons worried little about the role of gender in the diagnosis and treatment of flat feet. Instead, class and occupation were the primary concerns in their evaluation and prescriptions. 27 The orthopaedists saw a direct correlation between nursing and soldiering, for both occupations required a certain ‘class of person’ who could assume jobs that demanded ‘a greater number of hours on the feet’ than most white-collar jobs. 28 Here, orthopaedists demonstrate an awareness that changes in the industrial workplace had a direct bearing on their practice. In the new assembly-line factories of the early twentieth century—where Taylorism reigned and speed-ups were the norm—labourers had to stand in one place all day while conveyer belts and machines moved around them. These changes in the actual physical conditions of the factory floor resulted in serious repercussions for the labourer's body, as static standing often led to more wear and tear on the joints than did moving and lifting. The new material conditions of Taylorism brought about mass strikes, as well as individual worker unrest, most frequently expressed in the doctor's office, where it was hoped that tired and weary feet could be cured. 29
When the actual time came to examine the physical status of American recruits in April 1917, uniform standards for the measuring and diagnosing of flat feet did not exist. Orthopaedics surgeons disagreed vigorously on how best to examine the foot. Some surgeons insisted that the ‘pedograph’—an ink imprint on paper of the weight-bearing surface of the feet—was the most reliable diagnostic tool. (Figure 1 ). Others claimed that in addition to the pedograph, the examiner should rely on a ‘scaphoid scale’, using a ruler to draw a line connecting the internal malleolus (the bony protrusion of the inner ankle) to the distal end of the first metatarsal (the base of the big toe). This line, known then and today as ‘Feiss’ line', transects the scaphoid bone and flat foot is diagnosed when the bony marker falls one to one-and-a-half inches below the line. Still others claimed that flat feet could only be diagnosed properly with an X-ray image of the foot while it was in a shoe. 30
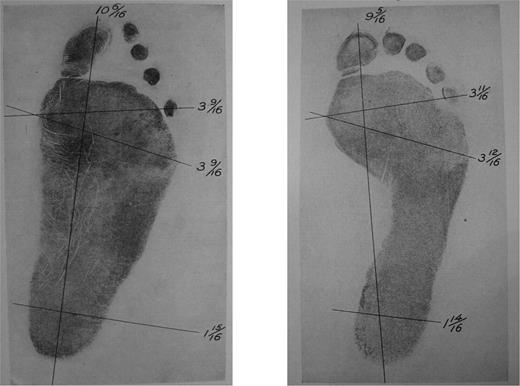
Pedography: Above left is a First World War pedographic example of flat feet, while above right is an imprint of a normally arched foot, evinced by the concavity of the instep. Source : Photographic reproductions are courtesy of the US National Archives and Records Administration, College Park, Maryland, Record Group 112, Box 430, file 730.
Despite the absence of standards at the outset of America's declaration of war, the US Medical Corps diagnosed thousands of recruits with the disorder. According to Philadelphia physician and Medical Corps orthopaedist, James T. Rugh, up to 25 per cent of the first group of soldiers examined had flat feet. Looking back on the figures a year later, Rugh speculated that only 3 per cent of the soldiers had ‘true’ flat feet and that the misdiagnosis of the condition was due to lack of military and orthopaedic experience on the part of a ‘majority’ of medical doctors. 31
With pressures coming from the military to control the steep numbers of men diagnosed with flat feet, and with charges of ‘misdiagnosis’ coming from all corners of the Medical Corps, the Division of Orthopedic Surgery led by Goldthwait, Osgood, Lovett and Brackett began in the winter of 1917 to talk in concrete terms about creating universal standards for diagnosis. The biggest hurdle that they faced was the fact that many examiners could not keep up with the speed of the military examination process. Rugh pushed his medical officers to ‘inspect 150–175 men in an hour’. 32 Another rank and file orthopaedic surgeon gave a relatively more sensible scenario, claiming that ‘two orthopedic surgeons and four clerks [could] examine and record the results of one hundred foot examinations per hour’. 33 If medical officers were indeed evaluating recruits at this rate, errors in diagnosis were bound to happen on a large scale.
Because of the time constraints put on the physicians who examined incoming recruits, the Division could not institute any sophisticated means of measuring for flat feet—all of the high-tech options were simply too time-consuming and highly contested. Thus the Division of Orthopedic Surgery decided to ‘cultivate the faculty of observation’ among all military medical officers. 34 While orthopaedists blamed the initial inflated numbers of flat feet on ‘average medical men’ who only glanced at the soldiers' arches, the leaders of the Orthopedic Division remained undeterred in their new emphasis on cultivating ‘observation’, for they felt that the physician's eye could be trained to evaluate feet with great precision. In short, orthopaedic surgeons aimed to educate, and in some cases ‘reeducate’, medical officers on the aesthetics of the foot as well as the entire body. 35
In order to get all military physicians to see the human foot in a uniform way, orthopaedic surgeons relied on the popular methods of physical anthropology of the day. To these wartime orthopaedists who had the opportunity to assess thousands of feet, the ideal foot was one that exhibited good form and obvious muscular strength. To better describe what this meant, orthopaedic surgeons identified two populations of people that were most likely to have perfect feet: young children and ‘savage, non-shoe-wearing’ people. 36 Taking their cue from Major Munson, First World War orthopaedists particularly liked using images of Filipino aboriginals—photographs commonly used to symbolise the US's achievements as a global, imperial power following the Philippine-American war (1898–1902)—in order to visually educate other physicians about the looks of the perfect foot. The Igorotes tribesmen, they argued, revealed a much desired ‘spreading of the forefoot’, a trait believed to improve a person's balance and endurance in work (Figure 2 ). 37
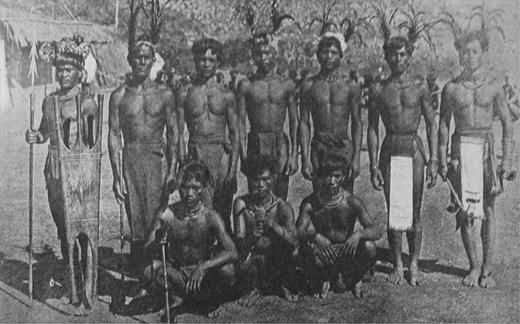
US Orthopedic surgeons used this photograph of Filipino aboriginals in order to standardise Army medical examinations of the feet. This image set the standard for the normal, ‘undeformed’ type of foot, made most apparent by the ‘spreading of the forefoot’. Source : Reproduced from Munson 1912 , p. 27.
Jim Crow laws and wartime segregation between black and white troops also informed and supported orthopaedists' anthropologically based assumptions. To them, the low-arch foot of black soldiers, while aesthetically unappealing, worked better under the strain and stress of war. In his post-war summary of foot efficiency, Brackett argued that ‘considerable differences exist among feet, between the high arch descendants of the Spaniard and the low arch of the negro’. 38 On the ground, many orthopaedic examiners working in Army training camps expressed astonishment that ‘Negro’ feet, while often looking flat, exhibited the greatest strength of all. Major E. W. Reyerson stationed in Army training camps in the American West and South begrudgingly admitted that African-American feet exhibited great strength under the physical demands of military life. As he reported, ‘we have had a large draft of negroes from Mississippi and Louisiana, who present the usual foot condition, a marked degree of flat foot, and it is surprising to see how many of these men can do as much marching as people with fine looking arches’. 39 That African Americans had better feet than the average white man did not, however, change the orthopaedists' white-supremacist view. For instance, Reyerson argued that his fellow orthopaedists should be thankful for the black man's strong foot since it was ‘more difficult to teach these rather indolent, mentally undeveloped [Negros] to use their feet properly’. 40
The blame for the high incidence of weak and flat feet among America's white soldiers thus rested on ‘civilisation’, or more precisely ‘over-civilisation’. While turn-of-the-century orthopedists, such as Whitman and Munson, targeted one part of civilisation—namely, industrialised shoe manufacturing—as the cause of flat feet, wartime orthopaedists used the notion of ‘civilisation’ in a far more generalised way, drawing on larger social and cultural fears that pervaded white America during the 1910s and 1920s. Indeed, Goldthwait, Brackett, Lovett, and Osgood invoked the term ‘civilisation’ in much the same way as other contemporary political and medical figures. Like Theodore Roosevelt and G. Stanley Hall, who worried about America becoming a nation of ‘soft’, ‘feminised’ civilians, wartime orthopaedists voiced concern about the prevalence of muscular weakness seen among the urban working class. Historian Gail Bederman has demonstrated that by the eve of America's involvement in the First World War, ‘civilisation’ became a highly charged term, infused with concrete assumptions about the intellectual and physical supremacy of the white man. The new white man of the 1910s promised to replace the Victorian man of self-restraint and gentility with a stronger and more physically virile ideal of manliness. The newer, stronger, ‘civilised’ man of the twentieth century would achieve the pinnacle of masculinity by combining the strength of the ‘racially primitive man’ with the intelligence and self-control of the civilised white man. 41
In keeping with this trend toward civilised masculinity, wartime orthopaedic surgeons praised ‘bare-footed savages’ as having ideal arches, perfectly formed feet, and beautifully shaped muscles. Consistent with the assumption that class mattered too, Brackett celebrated the foot ‘as it occurs among our [white] mountain people’. Although such a foot presented ‘a lower, broader’ arch, Brackett contended, its ‘strength was beyond question’. 42 Reyerson described a similar experience where white, rural farmers in the ‘West, following the plow and doing lots of daily work’ had highly functional feet, ‘much better feet than clerks and civilians’. 43 While some orthopaedists attributed the increased foot strength seen among blacks and white farmers to their occupations and their tendency to work barefooted, others claimed that the difference was based in theories of evolution, physiology and ultimately heredity. Arguing against the Whitmanian tradition of explaining flat feet as a structural deformity, Medical Corps Lieutenant Tom S. Mebane contended that African Americans had stronger feet because they overcompensated for their inherited ligamentous ‘flaccity’. Civilised white men, on the other hand, had ‘terse ligaments’ by nature, which, while supporting the foot, inhibited adequate muscle strength to support the arch. 44
Based on the considerations of class and race, orthopaedic surgeons pinned their hopes for a successful campaign to create ‘foot fit men’ on the white urban working class. Since, as the argument went, African Americans were uneducable and supposedly not wanting for stronger feet, orthopaedists gave themselves a rationale for ignoring foot problems among the black troops. They employed similar reasoning when discussing middle- and upper-class white elites. The ‘leisured’ class recruits, complained Rugh, could not be educated in proper foot care because they exhibited too much ‘pride in foot dress’. 45 Rugh wrote that the ‘typical’ male recruit who would ‘take the first opportunity to trade shoes with a comrade and keep on trading until he [got] a shoe small enough to fit his fancy, not his feet’. Those recruits who came from moneyed classes, argued Rugh, were frequently ‘unwilling to wear the regulation [military] shoe’. 46 Major R. Tunstall Taylor supported Rugh's analysis that fashion mattered most among the wealthier recruits, claiming that these men were ‘vainer than women’ and persistently ‘ask[ed] for a [shoe] size too small’. 47
Although the eradication of flat feet was a vision of physical and societal perfectionism, it was one with limits. Unlike eugenicists who wanted to sterilise the unfit and legislate the removal of ‘defectives’ from city streets, orthopaedists did not shun men with permanent disfigurements, flat feet, or missing limbs. 48 Indeed, their professional survival relied on a steady population of people who would either be born with physical deformities or acquire them in adulthood. Orthopaedists sought instead to educate the nation to accept disabled soldiers while also providing the injured with the tools to reintegrate back into civilian life as seamlessly as possible. They shared a common vision with other Progressive-era reformers who wanted to clean up urban areas, eradicate poverty, and create a safer, more efficient industrial workplace. What sets them apart from other reformers, however, was their belief that physical medicine could bring about these desired changes.
Military Flat-Foot Camps
To better institutionalise the orthopaedists' anthropologically based aesthetic and to prove that flat feet was a curable problem, orthopaedic surgeons convinced the US Army by January 1918 to give them full permission to open up and supervise specialised exercise programmes, known as ‘Flat-Foot Camps’. In these camps, orthopaedic surgeons became scientific managers, overseers of the molding, building and manufacturing of the soldier's body.
Goldthwait opened the first two foot camps abroad: one in Harschechamp, France and the other in Barville, France, each about six miles to the rear of the frontline. The original purpose of these camps, according to Goldthwait, was to train the soldiers on how ‘to use the body rightly, particularly the feet and backs’. 49 But the actual need for the camps stemmed from the fact that the initial American troops sent to France in the summer of 1917 had been accepted into the Army before Wilson instituted a formal ‘universal Draft’, and thus before ‘careful [medical] scrutiny’ of soldiers took place. 50 Goldthwait worried that such a group of ‘unfit’ men, ‘poorly trained bodies’, would have a ‘[negative] effect upon the French soldiers’ who believed that the American troops were ‘ready for combat duty’. 51
With the opening of the first camp in December 1917, Goldthwait moved away from the Munson–Whitman particularistic model of seeing the foot as a singular appendage operating on its own physical principles to a more holistic view of the foot as the linchpin of a strong and well-functioning physical body. By instituting a more observer-oriented physical examination to assess the feet—a process that included the taking of ‘silhouettes’ to evaluate the full-body posture and carriage of an individual—Goldthwait insisted that the feet were crucial indicators of a globally failing body, one that could not be used to the best of its mechanical ability (Figure 3 ).
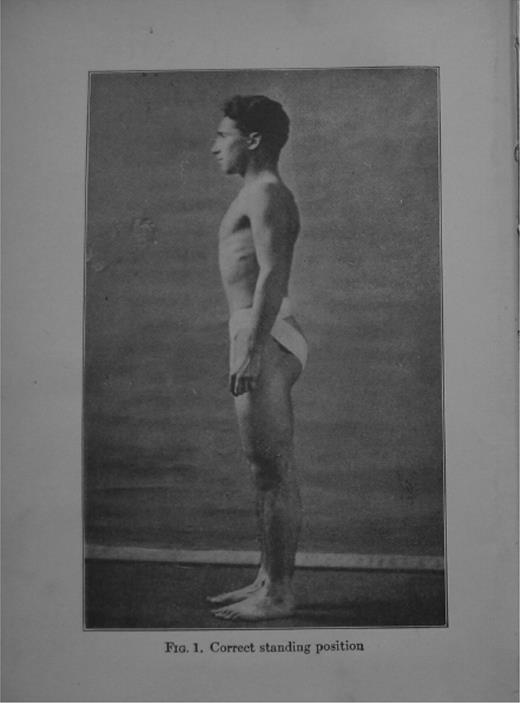
Body profiles, such as this, were often used to instruct other medical professionals, lay readers, and soldiers on how to stand properly so as to encourage arched feet rather than flat ones. Source : Reproduced from Thomas and Goldthwait 1922, front plate, opposite title page.
In the Flat-Foot Camps, Goldthwait and his personally trained line officers taught soldiers the mechanics of the body and feet through Army films, classroom instruction, and drills. Orthopaedists made flat feet into the potential Achilles heel of the US Army, repeatedly reminding the soldiers that ‘a sore-footed or weak man drags his company’ and that the US should be seen as nothing other than a country of ‘sound men’. 52 The safety, security, and strength of the country, the argument followed, rested not on the orthopaedic surgeons' capabilities as medical professionals, but rather on their ability as drill sergeant—and, more significantly, on the discipline and physical strength of the soldier himself.
Although orthopaedic surgeons still referred to themselves as ‘surgeons’ in the military chain of command, they rarely, if ever, performed operations, especially in the Flat-Foot Camps. Instead, self-proclaimed surgeons such as Goldthwait spoke in terms of the ‘reeducation’ of muscles and ‘vocational training’, arguing for the ‘reconstruction’ of defective men, not through the scalpel as one might expect, but rather through ‘drills’ and exercise to make damaged parts usable again. If necessary, orthopaedic surgeons in the camps would prescribe a figure-of-eight boot strap to a soldier to relieve persistent flat feet, but this was still not the preferred mode of treatment. To orthopaedists, the best way to cure the ‘unfit’ soldier was to make him physically strong, in every muscle of his body.
It is no surprise that Goldthwait built a wartime fleet of orthopaedic surgeons who voiced antipathy toward the knife. Since he began his professional career in the orthopaedic surgeon-directed medico-mechanical department at Massachusetts General Hospital (MGH), Goldthwait was far more versed in exercise prescription than in surgical techniques. Created in 1904, the MGH medico-mechanical department boasted a new approach to the treatment of fractures, arthritis and ‘back and feet cases’, a population of people that made up over 50 per cent of their patient load. 53 At the MGH, physicians treated painful limbs and joints through massage and hydrotherapy, as well as through the use of mechanical exercise equipment. Accordingly, the Boston-led team of wartime orthopaedists professed the values of conservative surgery. 54 While this vision left out the most acute stages of surgical care (i.e. securing fractured bones, manipulation of dislocated limbs, and the amputation of mutilated extremities), the Boston group was content to leave emergency care—the actual bloody work of cutting and sewing—to general surgeons.
Although surgical operations were gaining much prestige in civil society, the orthopaedists' adherence to conservativism paid off, especially in the wartime military milieu. Conservative orthopaedic surgery appealed to commanders engaged in battle who did not want surgeons performing ‘unnecessary’ surgeries on their infantry men and who argued that the military had neither the financial resources nor the reserves of manpower to allow for a long duration of convalescence among its fighting ranks. 55 Avoidance of liability was another concern. According to Rugh, ‘the question of corrective operations . . . should be approached with utmost caution’, for, he continued, ‘in civil life these operations would be relatively simple, but in military service there are many obstacles to success’, namely ‘the protection of the Government against unjust and false claims after the war is ended’. 56
By the time of the Argonne offensive—the strategic repositioning of American forces in September 1918 to the southern portion of the Western Front in response to planned enemy attacks on the Allied forces—the Flat-Foot Camps in Harschechamp and Barville closed. 57 The offensive demanded not only a great number of fighting soldiers, but also military personnel who could treat the thousands of American casualties coming out from the Argonne Forest. But although the US Army closed the camps abroad, the Flat-Foot Training camps remained alive and well at home under the direction of Brackett. Indeed, it was on the home front that orthopaedic surgeons fully developed and defined their profession as one interested not so much in therapeutic treatment, but rather in the prevention and prophylactic eradication of flat feet from the nation.
From War to Industry
The orthopaedic surgeons who supervised Flat-Foot Camps on American soil followed similar guidelines to those established abroad, yet they enjoyed the additional power of ‘eliminating the unfit’, rejecting ‘defective’ soldiers from military service entirely—a decision-making power that military psychologists, such as Robert Yerkes, never possessed. Flat-Foot Camps at home thus became an additional depot where soldiers would be examined and reexamined to assess their fitness level.
As the war progressed abroad, Flat-Foot Camps at home morphed into total body fitness camps. While these Flat-Foot Camps inevitably delayed thousands of American men from reaching the front-line as fast as they would have otherwise, the US Army nevertheless supported the programme, believing the orthopaedic surgeons' assessment that bodily muscle weakness was the single most ‘important factor in disability’ and inefficiency. 58 Once again, orthopaedic surgeons blamed the prevalence of muscular weakness on ‘civilisation’ and the urban workplace—on the fact that ‘large numbers of [recruits had] been engaged in sedentary pursuits, with little or no opportunity for outdoor activities’. 59
In essence, the orthopaedists and the US Army saw the Flat-Foot Camps as a way to shore up the public health of the nation's men, not simply for the purpose of creating stronger soldiers to send abroad, but more for the purpose of creating a stronger industrial workforce at home. Well before the war, both Osgood and Goldthwait spoke of orthopaedic surgery more as a commitment to the betterment of physical health and productivity than a medical specialty devoted to a particular anatomical part. In a 1916 issue of the Journal of the American Medical Association , Osgood contended that he and his colleagues could make all American working-class men into ‘happy, productive, wage earning citizens, instead of boastful, consuming, idle derelicts’. 60 Along similar lines, in his first ‘orthopaedic war preparedness report’, Goldthwait described orthopaedic surgery as a practice with a universal concern for ‘invalid men’, both in times of war and peace. 61 Such statements struck at the heart of common complaints heard in the US during the early twentieth century about the problems of poverty, of beggars on the street (a worry heightened by reports about the rise of street beggars in Europe as a result of the war), of extravagant military benefits given to Civil War veterans, and the decline in workplace productivity.
Reflecting the broader vision of orthopaedic surgery put forth by Goldthwait and Osgood, orthopaedic surgeons in charge of training camps at home began to refer to the soldiers with flat feet as ‘the inefficients’. 62 Throughout the war, orthopaedic surgeons, and especially Goldthwait, spoke in terms of aiding two armies: the military army as well as the so-called ‘Great Industrial Army’. Indeed, by the late 1910s and early 1920s, orthopaedists planned to take over industrial medicine entirely, or as Roland Hammond, chairman of the AMA Section on Orthopedics, put it, ‘to invade the field of industrial medicine’. 63 Employing the logic that a healthy worker automatically makes a happy worker, orthopaedic surgeons insisted that their programme in back and feet care would stave off social unrest and strikes among industrial workers.
The fact that orthopaedic surgeons at home began to refer to flat-footed soldiers as ‘inefficients’ and ‘non-productives’ evinces the degree to which industrial concerns shaped and influenced the practice of wartime orthopaedics. As historian Anson Rabinbach has demonstrated, the goal of modern European industrialists was to ‘eliminate the human resistance to perpetual work’—to eliminate, that is, human fatigue. 64 American industrialists held out similar hopes. They, too, wanted to rid the workplace of wasteful inefficiencies, especially those of the human kind.
Just as Taylorism and the science of management influenced how orthopaedic surgeons conceptualised the problem of flat feet at home, the orthopaedists' rather simple formula for creating a better nation through stronger feet appealed to and began to shape how American industrialists understood worker fatigue after the war. Toward the end of the First World War, many American industrialists became frustrated with university physiologists, who, funded by the US government through the National Research Council, took charge of solving the problem of worker fatigue. Historian Richard Gillespie argues that the physiologically based research in industrial fatigue declined immediately after the First World War because physiology ‘seemed to increase the complexity of [the problem]’, rather than providing a quick and practical solution. Industrialists remained unconvinced by the physiologists' ways of measuring fatigue, scientific trials that included everything from vascular skin-reaction and urine tests to blood pressure examinations. 65 Orthopaedic surgeons with their simpler, bio-mechanistic view of the body, on the other hand, offered a more understandable—and indeed more easily visualised—view of how to combat worker fatigue.
Unlike the physiologists who saw the body as a motor—a complex system of chemical combustion and the production of energy—orthopaedists relied more on the metaphor of the body as a machine, an organism of muscles and bones that functioned on the same principles as levers and pulleys. 66 In the First World War Flat-Foot Camps, orthopaedic surgeons tested and refined this vision of the human body almost by necessity; their vision of treatment relied on the education of all soldiers, many of whom had little more than a primary school education or were immigrants who were not fluent in spoken English. In these camps, orthopaedic surgeons described normal and flat feet as well as good and bad posture through visual demonstrations and classroom instruction. Basing their theory of fatigue on principles of anatomy rather than physiology, orthopaedic surgeons were able to convey their message to everyone from the line soldier (who, more often than not, became an industrial worker during times of peace) to the highest levels of management, civilian and military.
Immediately after the war ended, orthopaedists succeeded in using their military reputation and stature to secure a place in industrial medicine. By the early 1920s, many orthopaedic surgeons followed Goldthwait's lead into the new terrain of ‘biomechanics’. With his first edition of Body Mechanics and Health , Goldthwait created an exercise manual for the non-expert reader, outlining the most desirable posture, detailing the anatomy of the back and feet, as well as providing written and visual instructions on how to attain the most efficient mechanics of essential parts of the body (Figure 3). 67 Although the new theory of ‘biomechanics’ appeared comprehensive in intent, the feet still held a privileged position in orthopaedic discussions about proper body positioning and human bodily efficiency. In Goldthwait's book, for instance, the foot was the only anatomical part of the body to have a separate chapter of its own.
Flat Feet as a Social Problem
From the turn of the twentieth century to the end of the First World War, the diagnosis of flat feet came to be understood as not merely a medical problem, but also as a larger social problem, an indicator of national weakness, a kind of structural deformity endemic to the industrial workplace. Orthopaedists used the condition of flat feet to speak to larger political and social concerns of the day. They convinced their fellow middle-class Americans that flat feet was an indicator of racial decline of the white man, a threat to US industrial strength and productivity, and a potential drain on what most progressive Americans believed to be an already bloated Veteran Pension system. During the 1910s, the US government spent over 96 per cent of federal welfare dollars on its ageing population of Civil War veterans, most of whom never returned to work after their military service. Orthopaedic surgeons promised to put an end to this system of government hand-outs by rehabilitating defective and injured soldiers, putting them back into the workplace, and making them into wage-earning citizens. 68 With such political support, orthopaedic surgeons ascended to positions of great power, not simply as medical experts, but as scientific managers of the workplace, as guardians of the public health, and as protectors of US nationalism.
In doing so, orthopaedists engaged in the practice of social medicine. Their concerns about industrialism (and industrial warfare) linked them in an important way to their social medicine predecessors, such as James Philips Kay, Jules Guérin and Rudolf Virchow. But whereas nineteenth-century social medicine physicians responded to problems of disease created by industrialism (such as skin disease, respiratory disease, ophthalmic disease, occupational toxins, as well as conditions of the ear, nose and throat), orthopaedists concentrated on the disabilities that resulted from the war and workplace. 69
Under the rubric of social medicine, orthopaedic surgeons campaigned for the attainment of bodily perfection rather than for the control and avoidance of epidemic disease, for they understood physical disability to be as much of a threat to national health as germs. This focus on muscular efficiency was new within the sphere of public health, and, accordingly, the message was delivered through a broad array of institutionalised channels. In addition to the US Public Health Service, orthopaedic surgeons turned to the military, the industrial workplace and eventually the US Congress to get their message of health betterment heard. 70 As a result, flat feet become a well-recognised physical debility with a future by war's end.
Acknowledgements
I am especially grateful for the helpful suggestions of my thesis adviser, John Harley Warner. For their comments on earlier versions of this article, I wish to thank Roger Cooter, Glenda Gilmore, Susan Lederer, and Naomi Rogers.
Notes
‘Flat Foot, and other Foot Troubles’ 1919, pamphlet no. 12.
Office of the Surgeon General 1920.
Much of the archival work that informs this article took place at the US National Archives and Records Administration, College Park, Maryland. There is an abundance of correspondence, pedographs (see Figure 1), and exercise instruction guides relating to flat feet in Record Group 112, Box 430, file 730.
Winter 1980 , pp. 211–44.
Howell in Cooter et al. (eds) 1998, p. 85–105.
It should be noted that the word ‘flatfoot’ was part of the general American lexicon during this time period, most often used as a derogatory term to describe Irish cops and other undesirables of society. Irish-American fiction writer, James Farrell, captures this particular use of the term best in his Studs Lonigan Triology —a series of novels about Chicago's lower-middle-class Irish population in the early twentieth century. See Onkey 2005 . For a study on how Europeans understood flat feet to be a marker of Jewish racial inferiority, see Gilman 1991 , pp. 38–52.
American orthopaedic surgeons, like their British counterparts, were proponents of public health, bureaucratic statism, rationalisation, and scientific management. Roger Cooter provides the most comprehensive and compelling explanation for why scholars need to look beyond theories of professionalisation to understand how orthopaedic surgery was both a product and promoter of the modern state. See Cooter 1993 .
Indeed, one could even argue that they rejected surgery itself. For a survey of the surgical professions, and how each specialty relates to one another, see Lawrence (ed.) 1992. In this collection, see in particular, Brieger in Lawrence (ed.) 1992, to appreciate how rare it was for surgeons to be conservative in the early twentieth century. Pernick 1985 is also essential to understanding the dynamics and tensions between radical and conservative surgical theories in America leading up to the First World War.
For the most thorough history and definition(s) of social medicine, see Porter in Porter (ed.) 1997, pp.1–31, Porter and Porter 1988 , pp. 90–103. Marxists historians, such as E. Richard Brown, would most likely criticise orthopaedists for appealing to industrialists and their attempts to stabilise and appease labour through medical measures. See Brown 1979 .
To contend that wartime orthopaedics was more of a social idea than a medical specialty runs contrary to what many other medical historians and sociologists argue. For more on how orthopaedic surgery should be seen as a medical specialty, see Gritzer and Arluke 1985. See also Starr 1982 , Stevens 1998 , and Weisz 2006 .
Skipper and Hughes 1983, p. 1542.
Gillette 1994 , p. 158.
Ibid .
Rugh 1919 , p. 203.
Munson 1912 , pp. 34–5.
For more on Victorian era health reformers who advocated new styles of clothing, see Whorton 1982 .
Yosifon and Stearns 1998.
Whitman 1892 , p. 227.
Osgood 1911 , p. 418, emphasis in the original.
Osgood 1911 , p. 424.
According to Dr C. Hermann Bucholz of the Massachusetts General Hospital, 20 per cent of all cases seen by the medico-mechanical department between 1908 and 1914 were patients (presumably working class) with feet problems. See Bucholz 1914 , p. 1733.
For more on the history of the practice of fluoroscopy, see Duffin and Hayter 2000, pp. 260–82.
Cole et al. 1918, p. 61, and Rugh 1919 , p. 200.
Rugh 1918 , p. 536.
Mebane 1918 , p. 378.
Osgood 1925 , p. 70.
Ibid .
Orthopedic Council of the US Military 1918.
See Munson 1912 , p. 27, fig. 19. For more on how the US used images of Filipino aboriginals in the wake of the Philippine-American war to foster support for greater militarism and masculinity, see Hoganson 1998 .
Brackett 1927 , p. 598.
Major E. W. Reyerson in Rugh 1919 , p. 204.
Ibid .
Brackett 1927 , p. 597. For more on the importance of class as it related to flat feet, see Osgood 1911 , pp. 422–4.
Major E. W. Reyerson in Rugh 1919 , p. 204.
Mebane 1918 , pp. 378–9.
Rugh 1918 , p. 533.
Ibid .
Major R. Tunstall Taylor in Rugh 1919 , p. 203.
For more on ‘ugly law’ legislation and the practice of eugenic sterilization, see Pernick 1996 . Susan Schweik has also given several papers on this topic. See, for example, Schweik, ‘The American Ugly Laws’, American Association for the History of Medicine annual meeting, 1 May 2004, Madison, Wisconsin.
Goldthwait 1941 , p. 47.
Ibid . Wilson did not institute a draft until June 1917. Draft registration for the First World War began on 5 June 1917. See Keene 2001 .
Goldthwait 1941 , pp. 48–9.
Rugh 1918 , p. 532.
Bucholz 1914 , p. 1733.
For more on the history of conservative surgery, see Lawrence (ed.) 1992.
Rugh 1918 , p. 535.
Ibid .
Rugh 1918 , p. 431.
Brackett 1927 , p. 597.
Osgood 1916 , p. 418.
Goldthwait 1917 , p. 248.
Rugh 1918 , p. 431.
Cooter 1993 , p. 139.
Rabinbach 1990 , p. 2.
Gillespie in Geison (ed.) 1987, p. 249.
For a thorough description of the body-as-motor ideology, see Rabinbach 1990 .
Thomas and Goldthwait 1922.
Thomas and Goldthwait 1922, p. 61.
Several medical historians have portrayed the eugenics movement as the new social medicine of the twentieth century, whereby a ‘sound society’ was achieved through regulation of human reproduction. The best example of this argument can be found in Porter in Porter (ed.) 1997, and Porter and Porter 1988 . Although the eradication of flat feet was a vision of physical and societal perfectionism, it was not an effort to sterilise the unfit and legislate the removal of ‘defectives’ from city streets.
In 1918, the US Congress passed the Federal Vocational Rehabilitation Act which mandated that all injured soldiers receive both physical and vocational rehabilitation. For the story of how this legislative idea began and succeeded, see Linker 2006 .

{kind=link}
{kind=link}
{kind=link}