




Abstract
Responding to health needs in one disease area might rely on being able to draw on research and funding oriented towards other disease areas. However, the tendency of medical research to cross-disease areas has received limited empirical consideration. An outbreak, in a disease area with little prior research or funding, means that any research response will necessarily be rich with cross-disease flows. This affords a setting that allows us to identify and examine the phenomenon over time. We estimate the extent to which the vaccine research community’s response to Zika virus drew on research and funding from other diseases. We find that a persistently low share of funding into Zika vaccine research was Zika-oriented. In contrast, a much higher share of knowledge inputs was oriented to Zika. The exercise serves to illustrate some general themes in priority setting for health research systems alongside some core features of vaccine innovation.
1. Introduction
Disease outbreaks intensify hopes for a vaccine. The vision for a vaccine encompasses a wide range of stakeholders, even amidst much uncertainty about the disease (Blume 1992; Borup et al. 2006; Yaqub and Nightingale 2012). One response to disease outbreak is to draw on resources from other disease areas, in the form of research flows and funding flows across diseases. However, we know little about these two types of cross-disease flows.
An outbreak in a neglected disease area, with little prior research and funding oriented to that disease, means that any research response will necessarily be rich with cross-disease flows. This affords a setting that allows us to identify and track how long such flows might last and examine their distribution across disease areas to see where they originate.
One such case of research in response to an outbreak of disease with virtually no prior research or funding was Zika in 2016. Although the virus was discovered in 1947, and there were prior outbreaks in 2007 and 2013 (Osorio-de-Castro et al. 2017), the Zika vaccine literature emerged almost entirely after the Public Health Emergency of International Concern declaration in February 2016. Since 2016, approximately $350 m of research funding for Zika vaccine has been mobilised (Chapman et al. 2020: 18). However, before 2016, barely any investments were made; a search of US National Institutes of Health (NIH) RePORTER using the term ‘Zika’ returns no records of research funding at all. The comments of the Director of the US National Institute of Allergy and Infectious Diseases, for example, are instructive:
‘In the early stages, we just diverted people, money, resources, activity away from the standard things that we were doing to start working on a Zika vaccine… Then it became very clear, very quickly, that in order to really mount this effort including vaccine [and] other things, we would need additional resources’ (Fauci, in Rodriguez 2016).
The comment prompts at least two lines of enquiry. Firstly, from which disease areas were resources diverted in order to mount the initial crisis response and, secondly, for how long did this situation last until more Zika-oriented funding arrived? We might expect funding inputs and repurposed knowledge inputs for Zika vaccine research to come from neighbouring disease areas, unless capabilities are unevenly distributed across disease areas. Moreover, we might expect such cross-disease flows to rapidly recede into a minority share as Zika-oriented funding arrives and as Zika-specific knowledge is accumulated. In contrast to both these expectations, we find cross-disease flows from beyond neighbouring disease areas and that these flows remain over time.
2. Research priority setting and the sources of biomedical innovation
Where do resources to generate a widely appreciated technology, such as a vaccine, come from? Tracing the development of notable technologies back to their research inputs and other sources has a long tradition (Sherwin and Isenson 1967; IIT 1968; Rothwell et al. 1974; Comroe and Dripps 1976; Pavitt 1984). For biomedical innovation, debate often turns on whether sources come from public or private research, from basic or applied research, or from research or practice (Angell 2005; Nelson et al. 2011; Li et al. 2017)—but less often on whether they come from corresponding disease areas.
2.1 Disease as a vehicle for policy and practice
In health and medicine, researchers have highlighted the emergence of disease constituencies advocating for research on ‘their’ diseases (Dresser 1999; Hegde and Sampat 2015), donor programmes that favour a ‘vertical’ disease focus over broader health systems strengthening (Clinton and Sridhar 2017), and public–private partnerships that focus on specific products such as malaria vaccine or HIV vaccine (Chataway and Smith 2006; Chataway et al. 2010). Disease, as a category, is clearly relevant for policy and practice (Hacking 1995; Bowker and Star 1999; Rosenberg 2002; Jutel and Nettleton 2011).
Biomedical research funding is spread across multiple disease areas (as well as non-disease areas). The exact distribution of these funding allocations has attracted considerable scrutiny, not only in terms of which disease areas are afforded most funds but also in terms of the extent to which they are aligned with social priorities (as reflected by disease burden), local priorities (as reflected by geographical incidence), or political priorities (as reflected by advocacy activity) (Gross et al. 1999; Gillum et al. 2011; Evans et al. 2014). Where there seem to be misalignments between funding to a disease and its relative priority, advocates have used this as a basis for calls to change research funding allocations (Coburn et al. 2023).
Others, however, have argued that there ‘should not be absolute correspondence’ because a variety of factors—such as scientific opportunity, quality of research, and staffing—need to be considered in the allocation of funds across diseases (Varmus 1999: 1914; Lichtenberg 2001). In this view, misalignments between research priorities and disease priorities are a manifestation of the longstanding idea that ‘progress against disease results from discoveries in remote and unexpected fields’ (Bush, 1945: 14; Consoli et al. 2016; Yaqub, 2018).
These issues resonate with broader debates in the research policy literature on the extent to which it may be feasible and desirable to direct research investments in general towards particular outputs, outcomes, and social challenges (Sarewitz 1996; Mowery et al. 2010; Stilgoe et al. 2013; Ciarli and Ràfols 2019).
2.2 Disease outbreaks as a shock to the research system
Disease outbreaks may well be endogenous to modern socio-economic systems (Wood et al. 2012), but public policy reacts as if they were exogenous shocks:
‘Epidemics policy has largely adopted a “fast-twitch” approach to a problem that most agree has a “slow-twitch” causes: epidemics policy has become a policy of rapid response rather than long-term commitment’ (Dry 2008: 6).
This emphasis on rapid reaction can give rise to abrupt shifts in research funding and research outputs. The research response can be conceptualised as the redeployment of existing research capabilities to new problems, although these capabilities may not necessarily be located in the outbreak disease or even ones closely related to it. Over time, the response moves away from short-term repurposing activities and builds on newly accumulated knowledge and may therefore have longer-lasting impacts on epistemic structures and scientific communities.
As such, the tendency to respond to health needs in one disease area, specifically by drawing on research and funding oriented towards other disease areas, offers insights into the interconnected nature of medical research and its ability to respond to emergent demands. Mapping cross-disease flows in response to an outbreak would offer a window into whether the allocation of research funding across disease areas ought to consider the need to prepare research systems for future outbreaks—and, if so, to what extent.
A high share of cross-disease funding inputs would indicate dependence on funding from other disease areas for mounting an outbreak response. A persistently high share may indicate the slow arrival of new funds. This not only suggests a lack of preparedness for outbreaks in that disease area but also signals the long length of time needed for resource mobilisation for that disease constituency. Such evidence could be used to suggest that preparedness is well served by investing more evenly across a portfolio of diseases in advance of possible outbreaks (Wallace and Rafols 2015).
A high share of cross-disease knowledge inputs would indicate that the response drew on knowledge from other disease areas. A high share from distant disease areas may indicate situations where there is a prominent role for repurposed expertise. Such evidence could be used to suggest that, rather than focusing on the distribution of funds across diseases, preparedness is well served by investing in research capabilities and maintaining them (Price 1984; Teece et al. 1997).
3. Data and methods
We began by collecting all Zika vaccine publications between 2016 and 2019, to capture research done once that outbreak occurred. We examined antecedents of the corpus in two ways. We used publications cited by this corpus as knowledge inputs, and we used the project descriptions of the grant codes acknowledged by this corpus as funding inputs (Catalini et al. 2015; Grassano et al. 2017).
We then categorised these inputs to identify where there might be cross-category flows into the Zika vaccine corpus. We use a series of hierarchically nested categories (see section 3.3). This allowed cross-category contributions that were observable in the corpus to be considered in terms of differing degrees of ‘related variety’ (Frenken et al. 2007), distinguishing between proximate flows and more distant flows.
3.1 Collecting the Zika vaccine corpus
We searched PubMed (https://pubmed.ncbi.nlm.nih.gov/advanced/) for vaccine research with the Zika virus infection MeSH term, using the following query:
(‘2016/01/01’ [Date—Publication]: ‘2019/12/31’[Date—Publication]) AND (‘Zika virus infection’[MeSH Terms] AND (‘vaccines’[MeSH Terms] OR ‘immunization’[MeSH Terms])).
The query yielded 328 publications. We reviewed the full text of each in detail for two reasons: firstly, to be in a better position to understand the context of any cross-disease flows we might identify and, secondly, to guard against any publications in the corpus that might only be tangentially or superficially related to Zika. We determined that 16 were false, in fact not about Zika vaccine substantively. The exclusions were agreed upon across the three reviewers. This left a total of 312 publications in the 2016–9 Zika vaccine corpus.
3.2 Collecting funding inputs and knowledge inputs to the Zika vaccine corpus
We searched the 312 publications for funding acknowledgements, using the Web of Science, Scopus, NIH RePORTER, and UKRI-GtR. The reason for searching multiple sources is that funding acknowledgements can be incomplete in any given source. We found 776 acknowledgements but focused on cases where a specific grant or contract number was available.
With the grant numbers, we searched for information in the databases of 26 funders from across USA, China, Brazil, European Union (EU), UK, France, Canada, and Taiwan. These include NIH, National Natural Science Foundation of China, Ministry of Science and Technology China, EU, Fundação de Amparo á Pesquisa do Estado de São Paulo, Agence Nationale de la Recherche, Bill & Melinda Gates Foundation, UK Research and Innovation, and Wellcome Trust. We were able to locate descriptions for 256 unique projects from 533 acknowledgements. Project descriptions in Portuguese and Mandarin were retrieved by native speakers prior to translation. We gathered references cited by the Zika vaccine corpus using Web of Science.
3.3 Categorising funding inputs and knowledge inputs to the Zika vaccine corpus
We categorised each of the 256 project descriptions as being about Zika, about another disease, about a broad class of diseases, or non-disease focused. Coding reliability was assessed in a sample of 25 per cent of the projects, selected at random, and coded by three independent reviewers. Intercoder reliability was calculated across 2,838 observations, returning a kappa coefficient of 0.94 (at 95 per cent confidence level range of ±0.05) (Landis and Koch 1977). Further details are available below and in a supplementary annex.
This resulted in three mutually exclusive categories: no disease, disease oriented, and wide ranging for projects mentioning seven or more diseases. Disease-oriented projects were further coded into one or more individual diseases. Wide-ranging projects were coded into categories of increasing breadth: flavivirus diseases, arbovirus & RNA virus diseases, vector-borne & viral diseases, infectious diseases, and infectious & non-infectious diseases. These categories were based on the structure of the MeSH tree, a controlled vocabulary of Medical Subject Headings maintained by the US National Library of Medicine.
For the 12,304 references in the Zika vaccine corpus, it was not possible to categorise using manual review. Instead, we relied on the MeSH labels already assigned to these cited references. We found MeSH to be useful and reliable for this purpose. As already noted, in our original screening, we found 312 of the 328 articles that MeSH categorised as oriented to Zika vaccine were also Zika-oriented by our approach. We also manually reviewed some (250) of the references to explore their content. Moreover, by exploiting the structure of the MeSH tree, we could classify them with increasingly wider categories so as to mirror the approach used for projects as closely as possible.
4. Results
Using these data, we examined four questions about the orientation of funding inputs and knowledge inputs to the Zika vaccine corpus.
4.1 What share of funding inputs are oriented to Zika?
A low share of funding inputs to the corpus was Zika-oriented. In terms of projects acknowledged by the Zika vaccine corpus as a whole, only 14 per cent were oriented to Zika. To examine the dynamics of vaccine research funding inputs, the corpus was disaggregated by publication year (see Table 1).
Share of funding inputs that are Zika-oriented, over time.
| Share of projects acknowledged by the corpus that are Zika-oriented | |
|---|---|
| 2016 | 7% |
| 2017 | 14% |
| 2018 | 16% |
| 2019 | 21% |
| Share of projects acknowledged by the corpus that are Zika-oriented | |
|---|---|
| 2016 | 7% |
| 2017 | 14% |
| 2018 | 16% |
| 2019 | 21% |
Share of funding inputs that are Zika-oriented, over time.
| Share of projects acknowledged by the corpus that are Zika-oriented | |
|---|---|
| 2016 | 7% |
| 2017 | 14% |
| 2018 | 16% |
| 2019 | 21% |
| Share of projects acknowledged by the corpus that are Zika-oriented | |
|---|---|
| 2016 | 7% |
| 2017 | 14% |
| 2018 | 16% |
| 2019 | 21% |
We can see that the share of projects that were oriented to Zika remained low over time. It grew only from 7 per cent for publication year 2016 to 21 per cent for publication year 2019. Over the course of the outbreak, funding for Zika-oriented projects took an increasingly acknowledged role in the growth of the corpus, but at no point did it pass beyond a minority share of all acknowledged projects, even where one might have expected more targeted funds to have arrived.
We also observed a notable drop-off in publication frequency in the Zika vaccine corpus for the publication year 2019. Zika vaccine publications were more than halved between 2018 and 2019. This may be indicative of fading attention and neglect and suggests that the initial research response needs further directed funding if the response is to be consolidated and sustained.
These results clearly show that the Zika vaccine corpus emerged largely from non-Zika-oriented funding and, moreover, that this phenomenon was largely persistent over time. If the corpus did not emerge from Zika-oriented funding, then where did it emerge from? Results in the next section show that it emerged almost entirely from disease-oriented funding.
4.2 What are the main non-Zika funding inputs?
The main types of funding inputs in the Zika vaccine research effort were for projects oriented to other diseases (see Table 2). The vast majority of funding inputs to the corpus were oriented either to diseases or to a wide range of diseases (89 per cent). Relatively few of these were Zika-oriented. A small minority were not oriented to any disease (11 per cent). As anticipated in sections 1 and 2, this indicates an important role for disease-oriented funding and, in particular, cross-disease funding flows.
Share of funding inputs that are Zika-oriented.
| Share of projects acknowledged by the Zika vaccine corpus | |
|---|---|
| Disease-oriented | 63% |
| Zika-oriented | 14% |
| Wide disease range | 26% |
| No disease | 11% |
| Share of projects acknowledged by the Zika vaccine corpus | |
|---|---|
| Disease-oriented | 63% |
| Zika-oriented | 14% |
| Wide disease range | 26% |
| No disease | 11% |
Share of funding inputs that are Zika-oriented.
| Share of projects acknowledged by the Zika vaccine corpus | |
|---|---|
| Disease-oriented | 63% |
| Zika-oriented | 14% |
| Wide disease range | 26% |
| No disease | 11% |
| Share of projects acknowledged by the Zika vaccine corpus | |
|---|---|
| Disease-oriented | 63% |
| Zika-oriented | 14% |
| Wide disease range | 26% |
| No disease | 11% |
Whilst these non-Zika funding inputs were largely disease-oriented, they were unevenly distributed across a range of diseases (see Fig. 1).
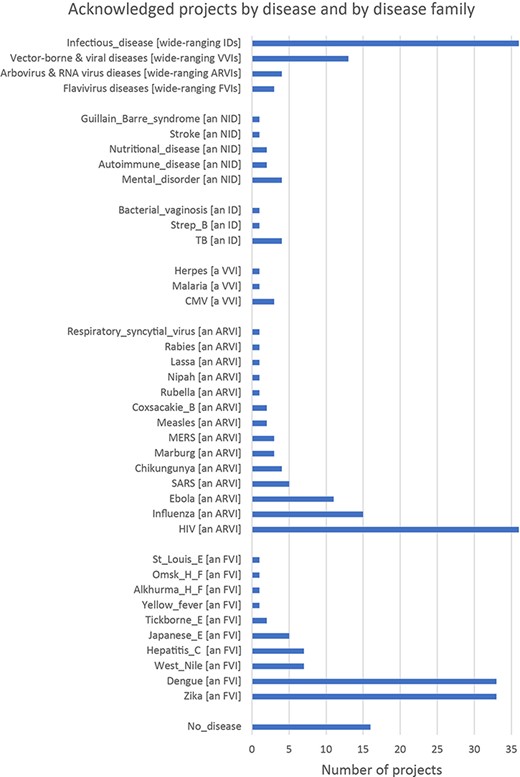
We can see that the most common disease orientations of acknowledged projects go beyond diseases in close proximity to Zika (flaviviruses). The five most frequent specific disease orientations of projects are HIV, dengue, Zika, influenza, and Ebola. Their project dates suggest that these were investments made in response to previous outbreaks. Ebola, Middle Eastern respiratory syndrome (MERS), influenza, severe acute respiratory syndrome (SARS), and HIV, each had outbreaks in 2015, 2014, 2009, 2002, and 1990s, respectively. HIV, in particular, was a longer-term outbreak with a sustained response.
The allocation of funds in response to prior disease outbreaks may have had long-lasting unseen effects on the research system that served as inputs into the research response to Zika. For example, two influential publications in the Zika vaccine corpus can be characterised as having been authored by HIV vaccine researchers and funded by HIV grants. The first of these showed protection against Zika virus challenge in mice with inactivated and DNA vaccine candidates (Larocca et al. 2016), whilst the second showed protection against Zika challenge in rhesus monkeys with inactivated, DNA, and viral-vector vaccine candidates (Abbink et al. 2016). They suggest researchers bringing HIV experience to bear on the Zika problem, not only in terms of techniques for developing promising vaccine candidates but also capabilities in developing animal models, handling challenge virus, measuring viral loads and immune response, and designing a three-way head-to-head study.
The results show that, whilst cross-disease flows appear to be proximate to Zika, some seem to be more distant from Zika. To explore disease proximity to Zika further and shed more light on the context of cross-disease funding flows, we present results in the next section from a manual review of the corpus, an analysis of its references in relation to the MeSH tree, and a sampling of some references for review.
4.3 What share of knowledge inputs are oriented to Zika?
To examine the dynamics of vaccine research knowledge inputs, the corpus was disaggregated by publication year. The top 100 publications cited by the corpus in a given year were gathered, manually reviewed, and classified as either Zika-oriented or not Zika-oriented. This revealed that the share of Zika-oriented publications cited by the corpus was high from the outset (see Table 3).
Share of knowledge inputs that are Zika-oriented, over time.
| Share of top 100 cited publications by the corpus that are Zika-oriented | |
|---|---|
| 2016 | 70% |
| 2017 | 87% |
| 2018 | 99% |
| 2019 | 94% |
| Share of top 100 cited publications by the corpus that are Zika-oriented | |
|---|---|
| 2016 | 70% |
| 2017 | 87% |
| 2018 | 99% |
| 2019 | 94% |
Share of knowledge inputs that are Zika-oriented, over time.
| Share of top 100 cited publications by the corpus that are Zika-oriented | |
|---|---|
| 2016 | 70% |
| 2017 | 87% |
| 2018 | 99% |
| 2019 | 94% |
| Share of top 100 cited publications by the corpus that are Zika-oriented | |
|---|---|
| 2016 | 70% |
| 2017 | 87% |
| 2018 | 99% |
| 2019 | 94% |
Even in the early stages of the outbreak, where one might have expected the corpus to draw on publications oriented to other diseases, there was still a strong preference for citing Zika-oriented publications. Specifically, this was a preference for citing what few Zika-oriented publications existed at the time. It suggests that explicit disease-specific knowledge was the prominent input to the corpus (although as noted, this does not preclude implicit repurposing of skills and capabilities).
These results provide a clear indication that some of the most influential knowledge inputs to the Zika vaccine corpus were also Zika-oriented. The next section offers an indication of the cognitive proximity of the remaining knowledge inputs and the extent to which they may be non-Zika-oriented.
4.4 What are the main non-Zika knowledge inputs?
Over three-quarters of non-Zika knowledge inputs to the Zika vaccine corpus were disease-oriented (see Table 4). The majority of these knowledge inputs to the corpus was Zika-oriented (i.e. not just the top 100 most cited as shown in the previous section). The median Zika vaccine publication had 45 per cent of its references oriented to Zika. For the Zika vaccine corpus as a whole, 5,918 of the 12,304 references (48 per cent) were to publications that have the Zika virus infection MeSH (ZVI MeSH) assigned to them.
Share of knowledge inputs that are Zika-oriented.
| Share of references in the Zika vaccine corpus | |
|---|---|
| Disease-oriented | 77% |
| Zika-oriented | 48% |
| No disease | 23% |
| Share of references in the Zika vaccine corpus | |
|---|---|
| Disease-oriented | 77% |
| Zika-oriented | 48% |
| No disease | 23% |
Share of knowledge inputs that are Zika-oriented.
| Share of references in the Zika vaccine corpus | |
|---|---|
| Disease-oriented | 77% |
| Zika-oriented | 48% |
| No disease | 23% |
| Share of references in the Zika vaccine corpus | |
|---|---|
| Disease-oriented | 77% |
| Zika-oriented | 48% |
| No disease | 23% |
Where citations were drawn from non-Zika material, these were still mostly disease-oriented. Of the 12,304 references, only 2,839 (23 per cent) were references to publications that are not disease-oriented (i.e. have no MeSH descriptors in C-branch). So, in terms of references to cited publications, the corpus exhibited a strong preference for citing Zika-specific material or disease-oriented material.
Whilst the main non-Zika knowledge inputs were disease-oriented, it appears that they were drawn from a narrow range of neighbouring disease areas, with 9,154 (74 per cent) references to infectious disease-oriented publications having at least one descriptor in the C01 infections branch. Figure 2 shows a disaggregation of the infections branch by assigning the references in a step-wise manner to increasingly tighter categories. We can see that most non-Zika references are oriented to flavivirus infections.
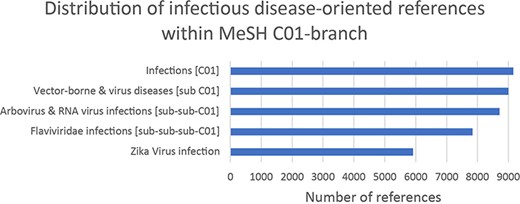
Distribution of non-Zika knowledge inputs.
Many references by the Zika vaccine corpus were reviewed in full text. Some were references to highly cited publications (more than 10,000 citations). These were invariably referencing particular techniques and methods. For example, analysis of gene expression using polymerase chain reaction (PCR) techniques and software tools to estimate phylogenies. Some references were frequently cited by the Zika vaccine corpus. Over a quarter of the Zika vaccine corpus cited publications reporting the structures of other flaviviruses with electron microscopy, and many others cited publications discussing cross-reactivity of antigens and clinical trial results.
Review of the Zika vaccine corpus also revealed non-Zika inputs for surmounting particular standardisation challenges. For example, ‘Individual vaccine projects, including our own, had to rely on internally developed clinical assays to understand vaccine-related immune responses and to detect prior or current infections. Lack of standardisation, however, can confound the interpretation of results from studies using different “home brew” assays across multiple laboratories such that study results cannot be directly compared in the absence of an accepted international standard or a proficiency panel of samples’ (Roberts 2019). This suggests a possible governance and co-ordination role for some non-Zika-specific resources.
Analysing both research projects and cited works in combination, we can see that the Zika vaccine corpus drew on a range of non-Zika-specific projects, but its citation behaviour was decidedly more Zika-specific. The results not only show cross-disease funding inputs but also show that some of these went beyond what might be considered neighbouring diseases.
5. Discussion
Responding to health research needs in one disease area with resources oriented towards other disease areas is an idea with limited evidence, partly because such cross-disease flows have been difficult to map and observe. Yet, diseases remain an important vehicle for policy and practice. Advocacy groups, research funding, and entire research institutes are often assembled around the notion of a disease. By focusing on an outbreak of disease with little prior funding and research, we have been able to identify and examine the phenomenon. In doing so, the exercise serves to illustrate some general themes for priority setting in medical research systems, particularly in relation to outbreak responsiveness and vaccine innovation.
5.1 Prompt research response, lacklustre funding to sustain it
The Zika vaccine research response initially had to draw on funds allocated to other diseases because there was such a paucity of Zika-oriented funding prior to 2016. As such, the vast majority of research grants acknowledged by the Zika vaccine corpus were oriented to diseases other than Zika. These seem to be cross-disease flows forged in crisis mode.
However, by tracking the phenomenon over time, we see that the tendency to draw on funding for other diseases is persistent and recedes only slightly as Zika-oriented funding is mobilised following the 2016 Public Health Emergency of International Concern declaration. In terms of the dynamics of cross-disease funding flows then, we find the situation to have been largely unchanging over time.
This may reflect the possibility that the arrival of Zika-oriented research funds after the 2016 PHEIC was too little or too late or both. The limited arrival of Zika-specific funds may have contributed to a slowdown in Zika vaccine research output. By 2019, Zika vaccine publication output slowed substantially, indicating fading attention. If Zika research was a neglected field prior to the outbreak, these results suggest that Zika vaccine research funding remained weak even after the outbreak.
As such, there may well have been researchers who were well suited to respond but were unable to do so because they could not be released from their existing commitments, did not have the scale of resources associated with large projects, or could not assemble teams and access the requisite networks.
The meagre funding response to the outbreak may have given rise to persistent cross-disease flows, but it also offers an opportunity to examine whether these cross-disease flows came from disease areas proximate to Zika or from disease areas more distant from Zika.
5.2 Cross-disease flows from neighbouring disease areas
An important challenge affecting how tentatively we might make sense of cross-disease flows is the nature of disease itself as a categorically distinct and independent entity (Hacking 1995; Bowker and Starr 1999; Rosenberg 2002). A single symptom may be related to a multitude of causes; conversely, a single cause may relate to a wide variety of symptoms. Zika as a disease is a case in point. Encephalitis and haemorrhagic fever are symptoms that cross disease. Zika is vector-borne but so too are malaria and leishmaniasis. Zika is sexually transmitted but so too are HIV and gonorrhoea. Diseases are a social constellation of causes and symptoms that in some cases are only loosely tied together with a diagnosis.
To account for some of these issues, our analysis used references to prior literature as a way of capturing knowledge flows, alongside full-text review. Publications cited by the corpus discuss cross-reactivity with dengue virus and a clinical trial of West Nile virus vaccine. Other cited publications highlight concerns about antibody-dependent enhancement, co-infection, and shared structural and membrane proteins across pathogens. One might consider these cross-disease flows to be a reasonable, perhaps even to be expected, reflection of the relationships, and interconnections between diseases in medical research.
Many cross-disease funding flows were between related families of pathogens and symptoms as exhibited in the literature we reviewed. These contributions to the response were supported by grants oriented to disease families related to Zika.
These cross-disease flows of knowledge and funding from neighbouring disease areas indicate broad-brush ‘correspondence’ with research funding targeted to diseases and would suggest that preparedness is well served by investing across a portfolio of disease families (Wallace and Rafols 2015).
However, whilst these cross-disease funding flows came from neighbouring disease areas, other contributions to the Zika vaccine corpus were more conspicuous and came from further afield.
5.3 Cross-disease flows from more remote disease areas
Some of the first responders offered contributions to the Zika vaccine corpus that seem to have drawn on investments made in response to prior disease outbreaks. That is, funding allocated in response to outbreaks of other diseases played a noticeable role in the emergence of the Zika vaccine corpus. Notable teams were supported by grants oriented to HIV and influenza. Some of these were large well-established teams and produced contributions that were highly cited by the Zika vaccine corpus.
This suggests that the quality of the response, in terms of requisite skills and accumulated capabilities, may not necessarily be located in proximate disease areas, but rather in the teams that have seen large and long-term prior investments. Furthermore, it appears that the legacy effects of prior outbreaks may be variable. For example, Ebola funding had an observable impact on the Zika vaccine corpus, although not as large as that of HIV funding.
Focusing on the tools and techniques available for redeployment, an additional way of interpreting cross-disease flows comes to light. Research capabilities can contribute to cross-disease funding flows from remote disease areas. These cross-disease flows from distant disease areas indicate an important role for research capabilities and would suggest that preparedness is also well served by investing in the maintenance of research capabilities for mounting a response (Price 1984; Teece et al. 1997).
The mixture of cross-disease funding flows from neighbouring and remote disease areas suggests a trade-off for policymakers when investing in research. A further role for cross-disease flows comes into view when we focus on moving vaccine research from publication outputs to innovation outputs.
5.4 Cross-disease flows are especially important for vaccine innovation
For the purposes of moving forward with developing and testing vaccines, cross-disease flows may be necessary; disease-specificity may even exert critical constraints.
In 2016, there seemed to be considerable potential for a vaccine: Zika virus presented relatively low variation, humans exhibited some degree of natural immunity, and reasonable animal models had been developed (Thomas et al. 2016; Yaqub, 2017b). However, in as little as 3 years later, much of that promise seemed to have dissipated. Firms withdrew their candidates from testing amidst a perception of greater market uncertainties and fewer testing opportunities as the epidemic waned (Branswell 2017). Public health successes and natural immunity can impede testing, and clinical trials need an epidemic that is not too fast but also not too slow (Yaqub, 2017a). It remains plausible that a ‘good’ Zika vaccine candidate was left on the shelf merely because it did not have a chance to prove its worth.
In this sense, the timeliness, scale, and agility of the funding response may be more significant than the disease-specificity of grants, as emphasised by the CEPI model and others (Røttingen et al. 2017; Hoffman and Silverberg 2018). To move vaccine research from publications to innovations, there is an important complementary role for timely, ‘disease-agnostic’ and ‘location-agnostic’ funding that can be mobilised to exploit the window of opportunity presented by outbreaks for testing vaccines.
Vaccine development funds would benefit from scale and scope, but they face three simultaneous challenges: (1) allocation to a ‘disease X’ that could be the next outbreak, rather than to a specific earmarked disease; (2) geographic flexibility, so that they may be deployed to wherever transmission is at its peak; and (3) preparedness, so that funds may be deployed within limited windows of outbreak opportunity.
Collectively, these are likely to pose tensions for disease constituencies, for global and local politics, and for public health systems strengthening. One recent and illustrative example can be found in the Chimpanzee Adenovirus Vector developed in the UK, Oxford. In previous guises, this was the basis for vaccine development efforts oriented to, in various turns, malaria, MERS, Crimean–Congo haemorrhagic fever, and Zika. Re-oriented to Covid-19, it was trialled in Brazil and other high transmission rate countries. It then formed the backbone of the vaccination programme for the UK and for much of the world. Notably, however, throughout these developments, there have been concurrent political pressures on parts of the UK’s research budget that are oriented to developing countries.
Vaccine innovation may be a case where funding targeted to disease categories exerts a constraining effect; disease categories may instead be more useful for indicating where market incentives are likely to be weak for certain vaccine products. This is because the market prospects for two vaccines based on identical techniques, but oriented to different diseases, can vary so greatly. This is significant because the costs of vaccine development can be much larger than vaccine research. Two vaccines based on identical techniques, but oriented to different diseases, entail generating two distinct sets of clinical trial evidence.
5.5 Conclusions
Responding to an outbreak with resources from the same or neighbouring disease areas offers a rationale for allocating research funds across a portfolio of disease areas. However, this is part of a trade-off because some skills and capabilities for responding to outbreaks may not necessarily reside in proximate areas, so there is a parallel rationale for allocating research funds to support the development and maintenance of research capabilities. The quality of these research capabilities underpins perhaps what is most prized about medical research during an outbreak, namely, its contributions to vaccine innovation.
In research priority setting, a relatively overlooked rationale for the allocation of research funds to particular diseases is that they might also, somewhat inadvertently, support the response to the next pandemic. Seen in this light, such investments are not only a response to a specific emergency, they also help to build resilience and capabilities in our research system, serving to strengthen an invisible infrastructure for public health. As our ability to respond is shaped by past research investments, it follows that the response now will shape our ability to respond in future.
Supplementary data
Supplementary data are available at SCIPOL Journal online.
Conflict of interest statement.
None declared.
Acknowledgements
We thank Bhaven Sampat and Ismael Rafols for their valuable comments. We thank Ramisha Rahman and Shih-Ya Chang for their excellent research assistance. We thank anonymous reviewers for their suggestions. We acknowledge European Research Council grant 759897, ESRC grant ES/L011409/1, and the British Council’s 2015 workshop on neglected diseases in Brazil.

{kind=link}
{kind=link}