




Abstract
Bridge employment has been encouraged by many countries worldwide as societies age rapidly. However, the health impact on bridge employment is not consistent in previous studies. This study aims to explore the association between bridge employment and long-term health outcome among the Chinese population.
In this prospective cohort study, we used a subset of the China Kadoorie Biobank study, in which 163,619 participants who reached the statutory age of retirement at baseline (2004–2008) were included in this study. Mortality statistics were obtained from death registries in the Death Surveillance Points system annually. We used a Cox proportional hazard model to analyze the association between bridge employment and all-cause mortality.
Overall, we found that compared to retired/nonemployed men and women, hazards of all-cause mortality were lower in older people with bridge employment (men: 0.82, 95% confidence interval [CI]: 0.77–0.88; women: 0.79, 95% CI: 0.74–0.94) in healthy populations. The protective effect of bridge employment was stronger among older adults living in rural areas and among those from a relatively low socioeconomic status.
The lower risk of all-cause mortality associated with bridge employment was consistently observed among older men and women. Our findings may provide important insights from the health dimension on the retirement policy-making in China as a hyper-aging society.
The increase in the population of aging people generally in developed countries and a few developing countries is contributing to the reduction of the working population and fiscal pressure on governments (Wu et al., 2016). China in particular is estimated to have 400 million older people by 2050, contributing to approximately 25% of the total older population worldwide (Lu, 2010). To alleviate the fiscal pressure, the United States elevated the age limit at which it is legal to obtain full retirement benefits from 65 to 67 (National Research Council and Institute of Medicine Committee on the Health Safety Needs of Older Workers, 2004), whereas the European Union eliminated compulsory retirement with the encouragement of older adults’ labor force participation (Cooke, 2006). China is similarly planning to raise the mandatory age for retirement of both labor and nonlabor workers (Feng et al., 2019).
There is an increasing trend of individuals turning to bridge employment. Bridge employment is defined as the labor force participation by older workers between career jobs and the complete withdrawal from the labor force (Wang et al., 2008). In Canada, 22% of retirees are estimated to return to work after their first retirement (Lecours et al., 2019). Furthermore, over 30% of American retirees are willing to possess a “second career” after retirement (Lecours et al., 2019). In developing countries, particularly in China with a relatively early statutory retirement age of 50 or 55 years for women, and 60 for men (Liu and Sun, 2016), 8.4% of adults aged 50 and older report to have paid work (Ko and Yeung, 2018).
Although most previous studies focused on predictors of bridge employment (Cahill et al., 2006; Maestas, 2010), the outcomes are rarely identified (Wang and Shultz, 2010), especially in developing countries. In addition to the benefits of bridge employment on late-life financial resources, daily activities, family relations, and social network (Vaupel and Loichinger, 2006), evidence of health impacts is also needed to justify the pursuit of bridge employment. Based on the Health and Retirement Study in older Americans, older adults with bridge employment were mentally and physically healthier than those who left labor work completely (Zhan et al., 2009). Another study reported the psychological benefits of bridge employment in older adults (Wang and Shi, 2014). However, these findings may be attributed to healthy worker bias, which refers to the fact that people with poor health are less likely to have bridge jobs (Maestas, 2010). Furthermore, the shortfall in studies focusing on bridge employment in developing countries calls for further evidence on health impacts of bridge employment from developing countries.
Therefore, this study aims to investigate the association of all-cause mortality with bridge employment among Chinese adults older than the mandatory age of retirement, taking into account of the healthy worker bias by separately investigating the associations in those with major conditions and those without.
Method
Study Design and Participants
The study was based on the baseline and long-term follow-up data of China Kadoorie Biobank, a population-based prospective cohort study in China. Its design, methods, and participants have been described in detail previously (Chen et al., 2005, 2011; Li et al., 2012). Information on the baseline and follow-up can be found in Supplementary Appendix 1.
The statutory age of retirement in China is 50 years for female workers, 55 years for female administrators, and 60 years for all males (The Fifth National People’s Congress of the People’s Republic of China, 1978a, 1978b). To ensure that all participants reached the retirement age, we excluded women participants younger than 55 years and men participants younger than 60 years (N = 349,272). No missing data were found during the analyses. The exclusion resulted in a total of 163,619 eligible participants.
Measures
Exposure
In the current research, either extending the current occupation or beginning a new job after reaching the mandatory retirement age was classified as bridge employment, while those who did not have a paid job at the time of survey were classified as nonemployment. In the baseline survey, participants were asked “What is your current occupation?” Then they were categorized into two groups: (a) bridge employment (“agriculture-related workers,” “factory-workers,” “administrator/manager,” “professional/technical,” “sales and service workers,” “self-employed,” and “others or not stated”) and (b) retirement/nonemployment (“retired,” “housewife/husband,” or “unemployed”).
Outcome
Vitals of study participants were monitored annually through local Disease Surveillance Points system and official residential records, which provided accurate and complete mortality statistics. The duration of follow-ups was calculated by using the time interval between the date of the baseline survey and the earliest among the following: date of death, loss of follow-up, or December 31, 2016.
Other covariates
In the baseline survey, sociodemographic characteristics collected included age, region (rural/urban), sex, education (illiterate and primary school, middle school, and high school and above), household income (<10,000 yuan, 10,000–19,999 yuan, ≥20,000 yuan), and marital status (married, widowed/separated/divorced, never married), self-reported physician-diagnosed morbidities, and lifestyle behaviors, including alcohol consumption (never, occasional, regular) and smoking status (never, occasional or ex-smoker, regular). Those without any of nine major conditions such as diabetes, hypertension, and cancer at baseline were classified as healthy. Body mass index (BMI) was calculated as weight (kg) divided by height squared (m2). BMI (kg/m2) values were classified into three categories: not overweight (BMI < 24.0 kg/m2), overweight (24 ≤ BMI < 28 kg/m2), and obese (BMI ≥ 28.0 kg/m2) based on the Chinese standard (Chen et al., 2004). Metabolic equivalent task (MET) values were applied in this study on a basis of the 2011 Compendium of Physical Activities to quantify daily activities of participants in the past 12 months (Ainsworth et al., 2011). Participants were also asked to rate their health status and due to the small proportion of excellent health, self-rated health (SRH) was categorized into three groups: excellent/good, fair, and poor.
Statistical Analyses
The basic characteristics of the study population were presented by employment status and sex, using means and standard deviations (SDs) for continuous variables and frequency distribution for categorical variables.
We calculated the death events per 100,000 person-years by sex, health status, and bridge employment. Univariable and multivariable Cox proportional hazard models were used to estimate the relationship between baseline employment status and all-cause mortality. In the multivariable analyses, potential confounders including socioeconomic variables (region, marital status, highest education, and household income) and lifestyle factors (smoking, alcohol consumption, and SRH) were included. Stepwise models were applied to investigate potential confounding effects of the covariates (data not shown). Adjusted population attributable fraction was calculated after running the multivariable models, by assuming all the participants to have bridge employment. In subgroup analyses, the associations were further stratified by age, region, education, household income, SRH, BMI categories, MET, smoking status, alcohol consumption while adjusting for covariates other than the stratification variable in the multivariable model. A test for interactions was conducted. We estimated survival probability for men and women according to health status and bridge employment using Kaplan–Meier plots.
Two-sided p < .05 was considered statistically significant. All analyses were performed using STATA version 14.0 (StataCorp, College Station, TX).
Results
Descriptive characteristics of the studied population by bridge employment status and sex are presented in Table 1. Detailed characteristics of bridge-employed participants by type of employment are presented in Supplementary Tables 1 and 2. The number of bridge-employed men (N = 28,444, 49.81%) and retired/nonemployed men (N = 28,659, 50.19%) was similar, while more women were retired or nonemployed (N = 66,364, 62.30%). The age of retired/nonemployed participants and their counterparts were similar. Among both men and women, we found that those who were bridge-employed tended to live in rural areas (men: 86.68%; women: 86.16%), have an annual household income of less than 10,000 yuan, receive primary school education or below, have a higher level of METs, and to be regular smokers. Bridge-employed participants were also less likely to be overweight or obese, or to have chronic illnesses.
Characteristics of Participants Older Than Mandatory Age for Retirement
| Men | Women | |||
|---|---|---|---|---|
| Characteristics | Bridge employment | Retirement and nonemployment | Bridge employment | Retirement and nonemployment |
| N = 28,444 | N = 28,659 | N = 40,152 | N = 66,364 | |
| Age (mean, SD) | 66.18 (4.24) | 67.81 (4.43) | 61.26 (5.02) | 64.18 (5.84) |
| Socioeconomic characteristics | ||||
| Region (%) | ||||
| Rural | 86.68 | 23.35 | 86.16 | 30.70 |
| Urban | 13.32 | 76.65 | 13.84 | 69.30 |
| Marital status (%) | ||||
| Married | 85.44 | 89.80 | 82.75 | 75.41 |
| Widowed/separated/divorced | 12.80 | 9.61 | 17.18 | 24.47 |
| Never married | 1.75 | 0.59 | 0.07 | 0.13 |
| Education (%) | ||||
| Illiterate and primary school | 81.13 | 43.30 | 91.7 | 67.12 |
| Middle school | 14.16 | 23.40 | 6.15 | 18.86 |
| High school and above | 4.71 | 33.30 | 2.15 | 14.02 |
| Household income, yuan (%) | ||||
| <10,000 | 49.14 | 19.12 | 48.62 | 26.76 |
| 10,000–19,999 | 22.06 | 33.92 | 23.38 | 31.56 |
| ≥20,000 | 28.80 | 46.95 | 28.00 | 41.69 |
| Lifestyle factors | ||||
| Body mass index, kg/m2 | ||||
| <24 | 75.62 | 52.62 | 61.47 | 47.84 |
| 24–28 | 20.49 | 36.73 | 29.01 | 35.57 |
| >28 | 3.88 | 10.65 | 9.51 | 16.59 |
| METs, hours/day | ||||
| < Mean MET | 36.33 | 92.14 | 29.23 | 89.16 |
| ≥ Mean MET | 63.67 | 7.86 | 70.77 | 10.84 |
| Smoking (%) | ||||
| Never | 13.25 | 24.46 | 88.34 | 93.40 |
| Occasional or ex-smoker | 25.91 | 36.45 | 6.06 | 3.09 |
| Regular | 60.84 | 39.09 | 5.60 | 3.50 |
| Alcohol consumption (%) | ||||
| Never | 29.97 | 28.59 | 66.62 | 71.05 |
| Occasional | 41.83 | 46.73 | 29.92 | 27.20 |
| Regular | 28.20 | 24.68 | 3.46 | 1.75 |
| Health status | ||||
| With illness (%) | 26.66 | 44.97 | 23.19 | 39.99 |
| Self-rated health level (%) | ||||
| Excellent/good | 43.84 | 40.29 | 40.02 | 34.07 |
| Fair | 45.13 | 47.92 | 45.30 | 51.87 |
| Poor | 11.03 | 11.78 | 14.68 | 14.06 |
| Men | Women | |||
|---|---|---|---|---|
| Characteristics | Bridge employment | Retirement and nonemployment | Bridge employment | Retirement and nonemployment |
| N = 28,444 | N = 28,659 | N = 40,152 | N = 66,364 | |
| Age (mean, SD) | 66.18 (4.24) | 67.81 (4.43) | 61.26 (5.02) | 64.18 (5.84) |
| Socioeconomic characteristics | ||||
| Region (%) | ||||
| Rural | 86.68 | 23.35 | 86.16 | 30.70 |
| Urban | 13.32 | 76.65 | 13.84 | 69.30 |
| Marital status (%) | ||||
| Married | 85.44 | 89.80 | 82.75 | 75.41 |
| Widowed/separated/divorced | 12.80 | 9.61 | 17.18 | 24.47 |
| Never married | 1.75 | 0.59 | 0.07 | 0.13 |
| Education (%) | ||||
| Illiterate and primary school | 81.13 | 43.30 | 91.7 | 67.12 |
| Middle school | 14.16 | 23.40 | 6.15 | 18.86 |
| High school and above | 4.71 | 33.30 | 2.15 | 14.02 |
| Household income, yuan (%) | ||||
| <10,000 | 49.14 | 19.12 | 48.62 | 26.76 |
| 10,000–19,999 | 22.06 | 33.92 | 23.38 | 31.56 |
| ≥20,000 | 28.80 | 46.95 | 28.00 | 41.69 |
| Lifestyle factors | ||||
| Body mass index, kg/m2 | ||||
| <24 | 75.62 | 52.62 | 61.47 | 47.84 |
| 24–28 | 20.49 | 36.73 | 29.01 | 35.57 |
| >28 | 3.88 | 10.65 | 9.51 | 16.59 |
| METs, hours/day | ||||
| < Mean MET | 36.33 | 92.14 | 29.23 | 89.16 |
| ≥ Mean MET | 63.67 | 7.86 | 70.77 | 10.84 |
| Smoking (%) | ||||
| Never | 13.25 | 24.46 | 88.34 | 93.40 |
| Occasional or ex-smoker | 25.91 | 36.45 | 6.06 | 3.09 |
| Regular | 60.84 | 39.09 | 5.60 | 3.50 |
| Alcohol consumption (%) | ||||
| Never | 29.97 | 28.59 | 66.62 | 71.05 |
| Occasional | 41.83 | 46.73 | 29.92 | 27.20 |
| Regular | 28.20 | 24.68 | 3.46 | 1.75 |
| Health status | ||||
| With illness (%) | 26.66 | 44.97 | 23.19 | 39.99 |
| Self-rated health level (%) | ||||
| Excellent/good | 43.84 | 40.29 | 40.02 | 34.07 |
| Fair | 45.13 | 47.92 | 45.30 | 51.87 |
| Poor | 11.03 | 11.78 | 14.68 | 14.06 |
Notes: METs = metabolic equivalent tasks; SD = standard deviation.
Characteristics of Participants Older Than Mandatory Age for Retirement
| Men | Women | |||
|---|---|---|---|---|
| Characteristics | Bridge employment | Retirement and nonemployment | Bridge employment | Retirement and nonemployment |
| N = 28,444 | N = 28,659 | N = 40,152 | N = 66,364 | |
| Age (mean, SD) | 66.18 (4.24) | 67.81 (4.43) | 61.26 (5.02) | 64.18 (5.84) |
| Socioeconomic characteristics | ||||
| Region (%) | ||||
| Rural | 86.68 | 23.35 | 86.16 | 30.70 |
| Urban | 13.32 | 76.65 | 13.84 | 69.30 |
| Marital status (%) | ||||
| Married | 85.44 | 89.80 | 82.75 | 75.41 |
| Widowed/separated/divorced | 12.80 | 9.61 | 17.18 | 24.47 |
| Never married | 1.75 | 0.59 | 0.07 | 0.13 |
| Education (%) | ||||
| Illiterate and primary school | 81.13 | 43.30 | 91.7 | 67.12 |
| Middle school | 14.16 | 23.40 | 6.15 | 18.86 |
| High school and above | 4.71 | 33.30 | 2.15 | 14.02 |
| Household income, yuan (%) | ||||
| <10,000 | 49.14 | 19.12 | 48.62 | 26.76 |
| 10,000–19,999 | 22.06 | 33.92 | 23.38 | 31.56 |
| ≥20,000 | 28.80 | 46.95 | 28.00 | 41.69 |
| Lifestyle factors | ||||
| Body mass index, kg/m2 | ||||
| <24 | 75.62 | 52.62 | 61.47 | 47.84 |
| 24–28 | 20.49 | 36.73 | 29.01 | 35.57 |
| >28 | 3.88 | 10.65 | 9.51 | 16.59 |
| METs, hours/day | ||||
| < Mean MET | 36.33 | 92.14 | 29.23 | 89.16 |
| ≥ Mean MET | 63.67 | 7.86 | 70.77 | 10.84 |
| Smoking (%) | ||||
| Never | 13.25 | 24.46 | 88.34 | 93.40 |
| Occasional or ex-smoker | 25.91 | 36.45 | 6.06 | 3.09 |
| Regular | 60.84 | 39.09 | 5.60 | 3.50 |
| Alcohol consumption (%) | ||||
| Never | 29.97 | 28.59 | 66.62 | 71.05 |
| Occasional | 41.83 | 46.73 | 29.92 | 27.20 |
| Regular | 28.20 | 24.68 | 3.46 | 1.75 |
| Health status | ||||
| With illness (%) | 26.66 | 44.97 | 23.19 | 39.99 |
| Self-rated health level (%) | ||||
| Excellent/good | 43.84 | 40.29 | 40.02 | 34.07 |
| Fair | 45.13 | 47.92 | 45.30 | 51.87 |
| Poor | 11.03 | 11.78 | 14.68 | 14.06 |
| Men | Women | |||
|---|---|---|---|---|
| Characteristics | Bridge employment | Retirement and nonemployment | Bridge employment | Retirement and nonemployment |
| N = 28,444 | N = 28,659 | N = 40,152 | N = 66,364 | |
| Age (mean, SD) | 66.18 (4.24) | 67.81 (4.43) | 61.26 (5.02) | 64.18 (5.84) |
| Socioeconomic characteristics | ||||
| Region (%) | ||||
| Rural | 86.68 | 23.35 | 86.16 | 30.70 |
| Urban | 13.32 | 76.65 | 13.84 | 69.30 |
| Marital status (%) | ||||
| Married | 85.44 | 89.80 | 82.75 | 75.41 |
| Widowed/separated/divorced | 12.80 | 9.61 | 17.18 | 24.47 |
| Never married | 1.75 | 0.59 | 0.07 | 0.13 |
| Education (%) | ||||
| Illiterate and primary school | 81.13 | 43.30 | 91.7 | 67.12 |
| Middle school | 14.16 | 23.40 | 6.15 | 18.86 |
| High school and above | 4.71 | 33.30 | 2.15 | 14.02 |
| Household income, yuan (%) | ||||
| <10,000 | 49.14 | 19.12 | 48.62 | 26.76 |
| 10,000–19,999 | 22.06 | 33.92 | 23.38 | 31.56 |
| ≥20,000 | 28.80 | 46.95 | 28.00 | 41.69 |
| Lifestyle factors | ||||
| Body mass index, kg/m2 | ||||
| <24 | 75.62 | 52.62 | 61.47 | 47.84 |
| 24–28 | 20.49 | 36.73 | 29.01 | 35.57 |
| >28 | 3.88 | 10.65 | 9.51 | 16.59 |
| METs, hours/day | ||||
| < Mean MET | 36.33 | 92.14 | 29.23 | 89.16 |
| ≥ Mean MET | 63.67 | 7.86 | 70.77 | 10.84 |
| Smoking (%) | ||||
| Never | 13.25 | 24.46 | 88.34 | 93.40 |
| Occasional or ex-smoker | 25.91 | 36.45 | 6.06 | 3.09 |
| Regular | 60.84 | 39.09 | 5.60 | 3.50 |
| Alcohol consumption (%) | ||||
| Never | 29.97 | 28.59 | 66.62 | 71.05 |
| Occasional | 41.83 | 46.73 | 29.92 | 27.20 |
| Regular | 28.20 | 24.68 | 3.46 | 1.75 |
| Health status | ||||
| With illness (%) | 26.66 | 44.97 | 23.19 | 39.99 |
| Self-rated health level (%) | ||||
| Excellent/good | 43.84 | 40.29 | 40.02 | 34.07 |
| Fair | 45.13 | 47.92 | 45.30 | 51.87 |
| Poor | 11.03 | 11.78 | 14.68 | 14.06 |
Notes: METs = metabolic equivalent tasks; SD = standard deviation.
During the 15 years of follow-up, 11,460 men and 10,308 women died. Supplementary Figure 1 shows the Kaplan–Meier survival estimation by sex, health status, and bridge employment. Larger fractions of all-cause mortality were attributed to retirement/nonemployment in populations with existing diseases (14.5% in men and 20.2% in women) than those without (7.2% in men and 12.7% in women). The direction of association between bridge employment and all-cause mortality changed in men after adjusting for potential confounders. Lower hazards of all-cause mortality associated with bridge employment were found in the healthy participants among both men and women (Table 2). Compared to those who were retired/nonemployed, the hazard ratios (HRs) for all-cause mortality in the healthy populations were 0.82 (95% confidence interval [CI]: 0.77–0.88) and 0.79 (95% CI: 0.74–0.94) for men and women who were bridge-employed, respectively. Similar associations were observed in people with chronic conditions.
Associations of Bridge Employment Situation With All-Cause Mortality and Adjusted Population Attributable Fraction (PAF) for Bridge Employment
| Cox model | |||||||
|---|---|---|---|---|---|---|---|
| N | Death events | Age-standardized mortality rate per 100,000 person-years | Crude HR (95% CI) | Adjusted HR (95% CI)a | % PAF (95% CI)d | ||
| Men | |||||||
| Healthyb | Retirement and nonemploymente | 15,770 | 2,706 | 1,698 | 1.0 | 1.0 | |
| Bridge employment | 20,860 | 3,972 | 1,907 | 1.11 (1.06, 1.17)** | 0.82 (0.77, 0.88)** | 7.2 (5.0, 9.3) | |
| Unhealthyc | Retirement and nonemploymente | 12,889 | 3,305 | 2,728 | 1.0 | 1.0 | |
| Bridge employmente | 7,584 | 2,097 | 2,953 | 1.09 (1.03, 1.15)** | 0.76 (0.71, 0.82)** | 14.5 (11.2, 17.7) | |
| Women | |||||||
| Healthyb | Retirement and nonemploymente | 39,823 | 3,302 | 653 | 1.0 | 1.0 | |
| Bridge employment | 30,839 | 2,224 | 599 | 0.86 (0.82, 0.91)** | 0.79 (0.74, 0.94)** | 12.7 (9.7, 15.6) | |
| Unhealthyc | Retirement and nonemploymente | 26,541 | 3,623 | 1,208 | 1.0 | 1.0 | |
| Bridge employment | 9,313 | 1,159 | 1,079 | 0.90 (0.84, 0.96)** | 0.73 (0.68, 0.79)** | 20.2 (15.9, 24.4) | |
| Cox model | |||||||
|---|---|---|---|---|---|---|---|
| N | Death events | Age-standardized mortality rate per 100,000 person-years | Crude HR (95% CI) | Adjusted HR (95% CI)a | % PAF (95% CI)d | ||
| Men | |||||||
| Healthyb | Retirement and nonemploymente | 15,770 | 2,706 | 1,698 | 1.0 | 1.0 | |
| Bridge employment | 20,860 | 3,972 | 1,907 | 1.11 (1.06, 1.17)** | 0.82 (0.77, 0.88)** | 7.2 (5.0, 9.3) | |
| Unhealthyc | Retirement and nonemploymente | 12,889 | 3,305 | 2,728 | 1.0 | 1.0 | |
| Bridge employmente | 7,584 | 2,097 | 2,953 | 1.09 (1.03, 1.15)** | 0.76 (0.71, 0.82)** | 14.5 (11.2, 17.7) | |
| Women | |||||||
| Healthyb | Retirement and nonemploymente | 39,823 | 3,302 | 653 | 1.0 | 1.0 | |
| Bridge employment | 30,839 | 2,224 | 599 | 0.86 (0.82, 0.91)** | 0.79 (0.74, 0.94)** | 12.7 (9.7, 15.6) | |
| Unhealthyc | Retirement and nonemploymente | 26,541 | 3,623 | 1,208 | 1.0 | 1.0 | |
| Bridge employment | 9,313 | 1,159 | 1,079 | 0.90 (0.84, 0.96)** | 0.73 (0.68, 0.79)** | 20.2 (15.9, 24.4) | |
Notes: CI = confidence interval; HR = hazard ratio.
aAdjusted for age, region (rural/urban), marital status, highest education, and household income, smoking, alcohol consumption, and self-rated health.
bHealthy was defined as without the following major chronic conditions: diabetes, coronary heart disease, stroke or transient ischemic attack, hypertension, emphysema/bronchitis, asthma, kidney disease, cirrhosis/chronic hepatitis, and cancer.
cUnhealthy was defined as with one or more of the abovementioned diseases at baseline.
dThe fraction of the mortality observed is attributable to participants not having bridge employment, with 95% CI.
eThe reference group of each gender is composed of people free from bridge employment.
**p < .01.
Associations of Bridge Employment Situation With All-Cause Mortality and Adjusted Population Attributable Fraction (PAF) for Bridge Employment
| Cox model | |||||||
|---|---|---|---|---|---|---|---|
| N | Death events | Age-standardized mortality rate per 100,000 person-years | Crude HR (95% CI) | Adjusted HR (95% CI)a | % PAF (95% CI)d | ||
| Men | |||||||
| Healthyb | Retirement and nonemploymente | 15,770 | 2,706 | 1,698 | 1.0 | 1.0 | |
| Bridge employment | 20,860 | 3,972 | 1,907 | 1.11 (1.06, 1.17)** | 0.82 (0.77, 0.88)** | 7.2 (5.0, 9.3) | |
| Unhealthyc | Retirement and nonemploymente | 12,889 | 3,305 | 2,728 | 1.0 | 1.0 | |
| Bridge employmente | 7,584 | 2,097 | 2,953 | 1.09 (1.03, 1.15)** | 0.76 (0.71, 0.82)** | 14.5 (11.2, 17.7) | |
| Women | |||||||
| Healthyb | Retirement and nonemploymente | 39,823 | 3,302 | 653 | 1.0 | 1.0 | |
| Bridge employment | 30,839 | 2,224 | 599 | 0.86 (0.82, 0.91)** | 0.79 (0.74, 0.94)** | 12.7 (9.7, 15.6) | |
| Unhealthyc | Retirement and nonemploymente | 26,541 | 3,623 | 1,208 | 1.0 | 1.0 | |
| Bridge employment | 9,313 | 1,159 | 1,079 | 0.90 (0.84, 0.96)** | 0.73 (0.68, 0.79)** | 20.2 (15.9, 24.4) | |
| Cox model | |||||||
|---|---|---|---|---|---|---|---|
| N | Death events | Age-standardized mortality rate per 100,000 person-years | Crude HR (95% CI) | Adjusted HR (95% CI)a | % PAF (95% CI)d | ||
| Men | |||||||
| Healthyb | Retirement and nonemploymente | 15,770 | 2,706 | 1,698 | 1.0 | 1.0 | |
| Bridge employment | 20,860 | 3,972 | 1,907 | 1.11 (1.06, 1.17)** | 0.82 (0.77, 0.88)** | 7.2 (5.0, 9.3) | |
| Unhealthyc | Retirement and nonemploymente | 12,889 | 3,305 | 2,728 | 1.0 | 1.0 | |
| Bridge employmente | 7,584 | 2,097 | 2,953 | 1.09 (1.03, 1.15)** | 0.76 (0.71, 0.82)** | 14.5 (11.2, 17.7) | |
| Women | |||||||
| Healthyb | Retirement and nonemploymente | 39,823 | 3,302 | 653 | 1.0 | 1.0 | |
| Bridge employment | 30,839 | 2,224 | 599 | 0.86 (0.82, 0.91)** | 0.79 (0.74, 0.94)** | 12.7 (9.7, 15.6) | |
| Unhealthyc | Retirement and nonemploymente | 26,541 | 3,623 | 1,208 | 1.0 | 1.0 | |
| Bridge employment | 9,313 | 1,159 | 1,079 | 0.90 (0.84, 0.96)** | 0.73 (0.68, 0.79)** | 20.2 (15.9, 24.4) | |
Notes: CI = confidence interval; HR = hazard ratio.
aAdjusted for age, region (rural/urban), marital status, highest education, and household income, smoking, alcohol consumption, and self-rated health.
bHealthy was defined as without the following major chronic conditions: diabetes, coronary heart disease, stroke or transient ischemic attack, hypertension, emphysema/bronchitis, asthma, kidney disease, cirrhosis/chronic hepatitis, and cancer.
cUnhealthy was defined as with one or more of the abovementioned diseases at baseline.
dThe fraction of the mortality observed is attributable to participants not having bridge employment, with 95% CI.
eThe reference group of each gender is composed of people free from bridge employment.
**p < .01.
The protective effect of bridge employment was consistent in most strata (Figure 1). Subgroup analyses showed significantly lower all-cause mortality in those who were bridge-employed in nearly all strata in men. Similarly, a protective effect of bridge employment on all-cause mortality was seen in women except for women with an education level of middle school and above. The association between bridge employment and all-cause mortality was more pronounced in both men (HR: 0.87, 95% CI: 0.80–0.94 for healthy men; HR: 0.87, 95% CI: 0.80–0.94 for unhealthy men) and women (HR: 0.82, 95% CI: 0.76–0.90 for healthy women; HR: 0.85, 95% CI: 0.77–0.94) whose METs were lower than the mean value.
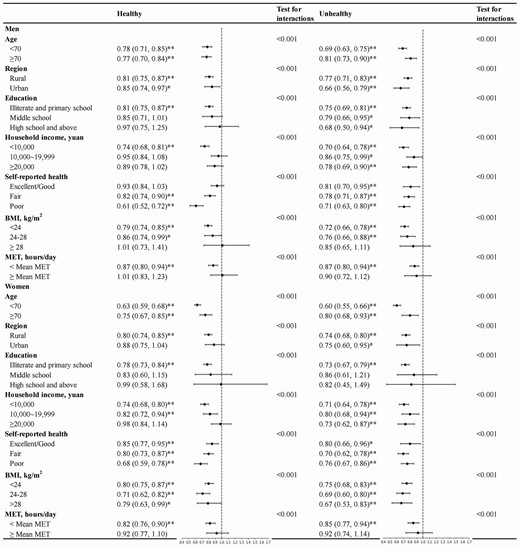
Stratified analysis of the association between bridge employment and all-cause mortality by sex (HR, 95% CI)†. †The reference group of each gender is composed of retired/nonemployed people, adjusting for age, region, marital status, highest education, household income, smoking, and alcohol consumption other than the stratified variable. *p < .05. **p < .01. CI = confidence interval; HR = hazard ratio.
Discussion
We found that a consistently lower risk of all-cause mortality was associated with bridge employment among older men and women at retirement age regardless of any major chronic conditions at baseline. Such a positive health effect of bridge employment appeared much stronger in older adults living in rural areas with a relatively lower socioeconomic status (SES). To the authors’ knowledge, this research is the first to examine the relationship between bridge employment in a large prospective cohort study in a Chinese population.
The finding that bridge employment was associated with lower risk of all-cause mortality was consistent with previous studies (Dave et al., 2008; Wu et al., 2016; Zhan et al., 2009). Three studies used data from the Health and Retirement Study conducted in the United States, while another one analyzed the association in Greece using the European Investigation into Cancer and Nutrition study (Zhan et al., 2009). One study that investigated the association between retirement age and all-cause mortality found the protective effects of later retirement consistent in both healthy and unhealthy retirees (Wu et al., 2016). In addition, the Greek study observed stronger relationship of bridge employment with mortality due to cardiovascular diseases than for mortality due to cancer, whereas they found no association for mortality due to injuries (Zhan et al., 2009).
The main finding of this study suggests a consistent health benefit of bridge employment regardless of chronic conditions. Bridge employment has been shown to be associated with fewer chronic diseases and functional limitations, and better mental health (Zhan et al., 2009). As a key component of an individual’s identity, employment could also provide people with financial security, psychosocial resources, and health insurance, which in turn improves their health status (Wu et al., 2016). Thus, retirees might consider their retired life stressful due to the loss of such resources (Elwell and Maltbie-Crannell, 1981). The current research also classified people who were unemployed as part of the reference group, and it is possible that mental stress and financial strain could influence their health.
There were confounding effects of socioeconomic factors, including region, education, and household income, on the observed association in men according to stepwise models. Participants with lower SES may experience higher economic strain and thus continue to work involuntarily after reaching retirement age. Additionally, they usually had poorer health than those with higher SES (Stringhini et al., 2017). Therefore, the crude estimates favored retirement and nonemployment. In our subgroup-stratified analyses, stronger associations were observed in rural participants and in those with a lower SES. The finding is consistent with a study conducted in Austria, which reported a similar association among male blue-collar workers (Kuhn et al., 2010). Mechanisms of such factors remain unexplained by present literature. One possible explanation might lie in the fact that lower SES populations are more likely to engage in work-related physical activity (Beenackers et al., 2012), which may contribute to better survival.
Strengths and Limitations
This is the first study to our knowledge that explored the associations between bridge employment and mortality in a developing country, using data from a large observational cohort study. The cohort provided detailed information on demographic, socioeconomic, lifestyle, physiological characteristics of participants, ensuring that this study rigorously accounted for the confounding effects of a person’s health status at baseline. We acknowledge several potential limitations. First, the questionnaire did not specify participants who were partially retired, or those who returned to work after baseline survey. However, we consider this as a random misclassification which might not affect the association. Second, the healthy worker selection effect may cause overestimation of the health benefits of bridge employment, as severe health conditions preclude the possibility of seeking bridge employment. Nevertheless, we conducted analyses stratified by health status and SRH. The consistent lower hazards of all-cause mortality associated with bridge employment suggest that the observed associations are less likely to be influenced by the healthy worker bias. Third, there is heterogeneity in the current classification of bridge employment and the reference group, which may complicate the associations. However, although due to different reasons, the retirees, housewife/husband, and unemployed people shared the same feature of not having formal occupations, leading to the emphasis upon the health benefits of continuity in participating in the workforce.
Research Implications
China is planning to gradually postpone the statutory retirement age (The 13th National People’s Congress of the People’s Republic of China, 2021). As a hyper-aging society, China can benefit from increased production attributed to longer duration of work and having more goods and services to provide for its people at all ages (Cahill et al., 2013). Individuals who delay their retirement will continue to play the role of taxpayers and thus help reduce the pecuniary burden of pension and social security for the aging society (Cahill et al., 2013). In addition to the benefits to the society, the impact of delaying retirement age on health must be taken into consideration. Our finding may have important policy implications from the health dimension in this context. Our study showed that continuing to participate in the workforce after reaching retirement age was at least not harmful to mortality. However, more evidence is needed to determine the optimal cutoff age that could maximize social productivity while considering the vulnerable group that is susceptible to afflictions due to prolonged work, especially those at risk of involuntary bridge employment (Dufouil et al., 2014). Similar to previous studies on bridge employment, the current research does not distinguish the types of bridge jobs, and therefore, future research is needed to explore if specific types of bridge jobs are more beneficial than others.
Conclusion
In conclusion, the lower risk of all-cause mortality was associated with bridge employment among older men and women at retirement age regardless of their health conditions. Our findings may provide important insights from the health dimension on the retirement policy-making in China as a hyper-aging society.
Funding
This work was supported by the National Key Research and Development Program of China (2016YFC0900500, 2016YFC0900501, and 2016YFC0900504); the Kadoorie Charitable Foundation in Hong Kong; and Wellcome Trust in the United Kingdom (088158/Z/09/Z and 104085/Z/14/Z). We are grateful for the Clinical Trial Service and Epidemiological Studies Unit, Nuffield Department of Population Health, University of Oxford, United Kingdom for providing the data. The authors received no support from any other organization for the submitted work.
Acknowledgments
We thank Chinese Center for Disease Control and Prevention, Chinese Ministry of Health, National Health and Family Planning Commission of China, and 10 provincial/regional Health Administrative Departments. The most important acknowledgment is to the participants in the study and the members of the survey teams in each of the 10 regional centers, as well as to the project development and management teams based at Beijing, Oxford, and the 10 regional centers.
Conflict of Interest
None declared.
Author Contributions
R. Y. Yin and Y. Q. Xin are joint co-first authors. K. Tang designed the study. R. Y. Yin and Y. Q. Xin conducted the study and analyzed the data. R. Y. Yin and Y. Q. Xin drafted the manuscript. K. Tang, R. Y. Yin, Y. Q. Xin, and Z. C. Wang contributed to the interpretation of the results. R. Y. Yin, K. Tang, Y. Q. Xin, M. Bhura, and Z. C. Wang contributed to revision of the manuscript. All authors have reviewed and approved the final manuscript.
References
Author notes
These authors contributed equally to this work.


{kind=link}