




Abstract
fall-related injuries constitute major health risks in older individuals, and these risks are projected to increase in parallel with increasing human longevity. Impaired postural stability is a potential risk factor related to falls, although the evidence is inconclusive, partly due to the lack of prospective studies. This study aimed to investigate how objective measures of postural sway predict incident falls.
this prospectively observational study included 1,877 community-dwelling individuals aged 70 years who participated in the Healthy Ageing Initiative between June 2012 and December 2015.
postural sway was measured during eyes-open (EO) and eyes-closed (EC) trials using the Wii Balance Board. Functional mobility, muscle strength, objective physical activity and cognitive performance were also measured. Participants reported incident falls 6 and 12 months after the examination.
during follow-up, 255 (14%) prospective fallers were identified. Division of centre of pressure (COP) sway lengths into quintiles revealed a nonlinear distribution of falls for EO trial data, but not EC trial data. After adjustment for multiple confounders, fall risk was increased by 75% for participants with COP sway lengths ≥400 mm during the EO trial (odds ratio [OR] 1.75, 95% confidence interval [CI] 1.09–2.79), and approximately doubled for sway lengths ≥920 mm during the EC trial (OR 1.90, 95% CI 1.12–3.22).
objective measures of postural sway independently predict incident falls in older community-dwelling men and women. Further studies are needed to evaluate whether postural sway length is of interest for the prediction of incident falls in clinical settings.
Introduction
Fall-related injuries are major health concerns for older individuals; they cause functional decline and increased mortality, as well as incurring vast healthcare costs for society [1–3]. Occurrences and consequences of falls are expected to increase globally with the growing number of older individuals. Hence, the improved detection of potential fall risk markers is of importance when predicting individuals at risk for falls and subsequently for improving strategies in fall-prevention.
Falling can be the end result of intrinsic and extrinsic factors negatively affecting an individual's ability to maintain balance [4], which are often revealed during sequences of body movement [5]. Balance can be dynamically and statically measured, the latter often involves having the individual in a stationary standing position, and researchers have from these measurements proposed impaired postural stability as a risk factor for falling [6, 7]. However, evidence regarding the association of postural instability with prospective falls is limited, and population-based cohort studies in this field are scarce [8]. Other shortcomings of previous studies include the use of retrospective study designs [9], which increase the risks of recall bias and the identification of risk factors as the result of falls [10, 11].
Postural instability is preferably investigated using objective measures of posturography, the advantages of which over regular clinical assessments include the reduction of test performance variability and avoidance of subjective scoring systems [12]. Recently, researchers have analysed the performance of the Wii Balance Board (WBB; Nintendo, Kyoto, Japan) in the measurement of postural instability; WBB-based assessment has shown excellent concurrent validity and the ability to complement existing fall assessments [13, 14]. However, these findings need to be evaluated in a population-based sample with a rich set of covariates. The current study was performed to investigate how objective measures of postural sway predicted prospective falls in a cohort of more than 1,800 community-dwelling men and women, all of whom were 70 years of age at the time of the investigation.
Methods
Study sample and ethical approval
This study was part of the Healthy Ageing Initiative, currently in progress at Umeå University, Sweden. Details of the study procedure have been described previously [15]; information is also available at www.healthyageinginitiative.com. To be included, participants had to live in the Umeå municipality and be 70 years of age at the time of examination. The sample for this study consisted of 1,877 community-dwelling individuals (914 women, 963 men) with complete measurements of postural stability and follow-ups on prospective falls. This study was approved by the Umeå University Research Ethics Committee and followed the precepts outlined in the World Medical Association's Declaration of Helsinki.
Assessment of postural stability
Postural stability was assessed using a WBB device labelled ‘Nintendo RVL-WBC-01’, with a nominal sampling frequency of 100 Hz. The equipment was linked to a personal computer via Bluetooth connection ‘E1310E(00**)’ using drivers labelled ‘Manage Library for Nintendo's Wiimote v1.7.00 by Brian Peek’. The software used for the assessment was designed in Microsoft C# (Microsoft; Redmond, WA, USA). The equipment's power supply was converted from battery to Universal Serial Bus.
Each participant conducted two 60-s trials in a quiet stance, consisting of eyes-open (EO) and eyes-closed (EC) conditions. Participants were instructed to maintain an upright position throughout the test, stand relaxed and avoid any arm or head movement. The WBB measured total centre of pressure (COP) sway length, representing the sum of postural sway in the anteroposterior and mediolateral directions. For comparison purposes, 104 participants performed identical measurement trials using the previously evaluated BioSway Balance System (BBS; Biodex, New York, NY, USA) [16]. The standard deviations of the stability indices obtained in these trials were used to match total COP sway lengths from the WBB.
Assessment of physical activity and capacity
Physical activity (PA) was measured objectively using triaxial accelerometers (GT3X+; Actigraph, Pensacola, FL, USA), which participants wore on the hip for 7 consecutive days. Instructions given to participants and accelerometer settings used for this study have been described previously [17]. PA was investigated using total activity counts, calculated by combining accelerations along all three axes and presented as daily averages. Participants also completed the Timed-Up-and-Go (TUG) test, commonly used by clinicians to assess lower leg muscle strength, gait performance and overall functional mobility [18]. Isometric muscle strength was tested by using a hydraulic hand dynamometer (Jamar; Patterson Medical, Warrenville, IL, USA) to measure each participant's maximum grip strength in the non-dominant hand. Participants were instructed to keep the arm at a 90° angle and to maintain the elbow in proximity to the waist during the test. The maximum value obtained in two consecutive attempts was recorded.
Prospective fall data collection
Participants reported potential incident falls when contacted by a research nurse 6 and 12 months after the examination. They were asked: ‘During the past 6 months, have you experienced a fall at the same level?’ Qualifying falls were defined as low-energy events in which participants came to rest on the ground unexpectedly by themselves.
Covariates
Anthropometric data were obtained using a scale (HL 120; Avery Berkel, Fairmont, MN, USA) to measure weight, and a gauge (Holtain Limited; Crymych, Dyfed, UK) to measure height. Participants also took the Mini-Mental-State Examination (MMSE), a common clinical test of cognitive functioning with a maximum score of 30 [19]. Participants self-reported any history of falls, cardiovascular disease (CVD) consisting of myocardial infarctions and stroke, and/or smoking.
Statistical analysis
Descriptive data were presented as means ± standard deviations, and Student's t-test was used to examine differences in study variables between fallers and non-fallers. Categorical variables were investigated using chi-squared tests. Pearson's correlation coefficient (r) was used to compare the results of postural sway trials and to investigate associations between data obtained from the two balance platforms. Data on postural sway from EO and EC trials were divided into quintiles to visualise the distribution of incident falls over COP sway length. Independent predictors of incident falls were investigated using multiple logistic regression models. The first model investigated only the sway parameters as independent predictors of incident falls, while the second and fully adjusted model included sex, weight, grip strength, PA, TUG test results, MMSE score, retrospective falls and CVD and smoking histories. Test-retest reliability was assessed using a two-way mixed effects model, with reporting of intraclass coefficients (ICC3,1) values for average measures. All analyses were performed with Stata software (version 13.1; StataCorp, College Station, TX, USA).
Results
Study cohort characteristics
In this study, 255 (~14%) participants reported falling at least once between the examination and follow-up timepoints. The majority (54.5%) of these fallers were women (P = 0.046). While fallers were more prone to report a history of falls (P = 0.001), fallers and non-fallers did not differ in terms of anthropometric characteristics, smoking, CVD history or MMSE score (Table 1). In terms of physical capacity and PA, fallers had less grip strength (P = 0.002) and poorer TUG test performance (P = 0.002) than did non-fallers, while also showing a tendency towards lower total PA per day (P = 0.057; Table 1).
Study cohort characteristics and comparisons based on incident falls
| Characteristic | All (n = 1,877) | Non-fallers (n = 1,622) | Fallers (n = 255) | P* |
|---|---|---|---|---|
| Covariates | ||||
| Age (years) | 70 | 70 | 70 | – |
| Women (%) | 48.69 | 47.78 | 54.51 | 0.046 |
| Weight (kg) | 77.30 ± 14.37 | 77.23 ± 14.32 | 77.73 ± 14.73 | 0.603 |
| Height (cm) | 170.22 ± 8.97 | 170.33 ± 8.92 | 169.54 ± 9.25 | 0.192 |
| Smoker, yes (%) | 6.03 | 6.30 | 5.10 | 0.456 |
| CVD, yes (%) | 9.94 | 9.71 | 13.47 | 0.071 |
| Previous fall, yes (%) | 31.99 | 30.74 | 41.15 | 0.001 |
| MMSE score | 28.44 ± 1.66 | 28.43 ± 1.67 | 28.48 ± 1.61 | 0.700 |
| PA/capacity | ||||
| Total activity per day (counts*1,000) | 466.66 ± 181.21 | 469.85 ± 181.09 | 445.98 ± 181.01 | 0.057 |
| Grip strength (kg, n) | 34.71 ± 10.93 | 35.02 ± 10.92 | 32.72 ± 10.82 | 0.002 |
| TUG test time (s) | 9.93 ± 2.28 | 9.84 ± 2.01 | 10.55 ± 3.46 | 0.002 |
| Postural sway | ||||
| EO COP sway length (mm) | 338.23 ± 133.41 | 333.80 ± 127.26 | 366.40 ± 164.78 | 0.003 |
| EC COP sway length (mm) | 735.31 ± 422.70 | 721.79 ± 400.47 | 820.64 ± 535.58 | 0.005 |
| Characteristic | All (n = 1,877) | Non-fallers (n = 1,622) | Fallers (n = 255) | P* |
|---|---|---|---|---|
| Covariates | ||||
| Age (years) | 70 | 70 | 70 | – |
| Women (%) | 48.69 | 47.78 | 54.51 | 0.046 |
| Weight (kg) | 77.30 ± 14.37 | 77.23 ± 14.32 | 77.73 ± 14.73 | 0.603 |
| Height (cm) | 170.22 ± 8.97 | 170.33 ± 8.92 | 169.54 ± 9.25 | 0.192 |
| Smoker, yes (%) | 6.03 | 6.30 | 5.10 | 0.456 |
| CVD, yes (%) | 9.94 | 9.71 | 13.47 | 0.071 |
| Previous fall, yes (%) | 31.99 | 30.74 | 41.15 | 0.001 |
| MMSE score | 28.44 ± 1.66 | 28.43 ± 1.67 | 28.48 ± 1.61 | 0.700 |
| PA/capacity | ||||
| Total activity per day (counts*1,000) | 466.66 ± 181.21 | 469.85 ± 181.09 | 445.98 ± 181.01 | 0.057 |
| Grip strength (kg, n) | 34.71 ± 10.93 | 35.02 ± 10.92 | 32.72 ± 10.82 | 0.002 |
| TUG test time (s) | 9.93 ± 2.28 | 9.84 ± 2.01 | 10.55 ± 3.46 | 0.002 |
| Postural sway | ||||
| EO COP sway length (mm) | 338.23 ± 133.41 | 333.80 ± 127.26 | 366.40 ± 164.78 | 0.003 |
| EC COP sway length (mm) | 735.31 ± 422.70 | 721.79 ± 400.47 | 820.64 ± 535.58 | 0.005 |
Values are presented as means ± standard deviations, except when percentages are displayed.
*Non-fallers versus fallers.
Study cohort characteristics and comparisons based on incident falls
| Characteristic | All (n = 1,877) | Non-fallers (n = 1,622) | Fallers (n = 255) | P* |
|---|---|---|---|---|
| Covariates | ||||
| Age (years) | 70 | 70 | 70 | – |
| Women (%) | 48.69 | 47.78 | 54.51 | 0.046 |
| Weight (kg) | 77.30 ± 14.37 | 77.23 ± 14.32 | 77.73 ± 14.73 | 0.603 |
| Height (cm) | 170.22 ± 8.97 | 170.33 ± 8.92 | 169.54 ± 9.25 | 0.192 |
| Smoker, yes (%) | 6.03 | 6.30 | 5.10 | 0.456 |
| CVD, yes (%) | 9.94 | 9.71 | 13.47 | 0.071 |
| Previous fall, yes (%) | 31.99 | 30.74 | 41.15 | 0.001 |
| MMSE score | 28.44 ± 1.66 | 28.43 ± 1.67 | 28.48 ± 1.61 | 0.700 |
| PA/capacity | ||||
| Total activity per day (counts*1,000) | 466.66 ± 181.21 | 469.85 ± 181.09 | 445.98 ± 181.01 | 0.057 |
| Grip strength (kg, n) | 34.71 ± 10.93 | 35.02 ± 10.92 | 32.72 ± 10.82 | 0.002 |
| TUG test time (s) | 9.93 ± 2.28 | 9.84 ± 2.01 | 10.55 ± 3.46 | 0.002 |
| Postural sway | ||||
| EO COP sway length (mm) | 338.23 ± 133.41 | 333.80 ± 127.26 | 366.40 ± 164.78 | 0.003 |
| EC COP sway length (mm) | 735.31 ± 422.70 | 721.79 ± 400.47 | 820.64 ± 535.58 | 0.005 |
| Characteristic | All (n = 1,877) | Non-fallers (n = 1,622) | Fallers (n = 255) | P* |
|---|---|---|---|---|
| Covariates | ||||
| Age (years) | 70 | 70 | 70 | – |
| Women (%) | 48.69 | 47.78 | 54.51 | 0.046 |
| Weight (kg) | 77.30 ± 14.37 | 77.23 ± 14.32 | 77.73 ± 14.73 | 0.603 |
| Height (cm) | 170.22 ± 8.97 | 170.33 ± 8.92 | 169.54 ± 9.25 | 0.192 |
| Smoker, yes (%) | 6.03 | 6.30 | 5.10 | 0.456 |
| CVD, yes (%) | 9.94 | 9.71 | 13.47 | 0.071 |
| Previous fall, yes (%) | 31.99 | 30.74 | 41.15 | 0.001 |
| MMSE score | 28.44 ± 1.66 | 28.43 ± 1.67 | 28.48 ± 1.61 | 0.700 |
| PA/capacity | ||||
| Total activity per day (counts*1,000) | 466.66 ± 181.21 | 469.85 ± 181.09 | 445.98 ± 181.01 | 0.057 |
| Grip strength (kg, n) | 34.71 ± 10.93 | 35.02 ± 10.92 | 32.72 ± 10.82 | 0.002 |
| TUG test time (s) | 9.93 ± 2.28 | 9.84 ± 2.01 | 10.55 ± 3.46 | 0.002 |
| Postural sway | ||||
| EO COP sway length (mm) | 338.23 ± 133.41 | 333.80 ± 127.26 | 366.40 ± 164.78 | 0.003 |
| EC COP sway length (mm) | 735.31 ± 422.70 | 721.79 ± 400.47 | 820.64 ± 535.58 | 0.005 |
Values are presented as means ± standard deviations, except when percentages are displayed.
*Non-fallers versus fallers.
Postural sway
Postural sway parameters from EO and EC trials differed between fallers and non-fallers (Table 1). COP sway length was significantly greater among fallers (P = 0.003), showing an approximately 10% difference from that of non-fallers during the EO trial. Similar results were obtained for the EC trial, although postural sway was generally higher in both groups compared with the EO trial (Table 1). In the EC trial, COP sway length was, on average, 14% greater in fallers than in non-fallers (P = 0.005). Furthermore, COP sway lengths from the two trials were strongly correlated (r = 0.64, P < 0.001).
Distribution of incident falls
In contrast to the EC trial, the EO trial revealed a potential nonlinear relationship between the distribution of falls and COP sway length, with a markedly increased frequency of falls in the 5th quintile (COP sway length ≥400 mm in EO trial, ≥920 mm in EC trial; Figure 1). All five quintiles of postural sway during both trials were subsequently added as independent predictors of incident falls to logistic regression models.
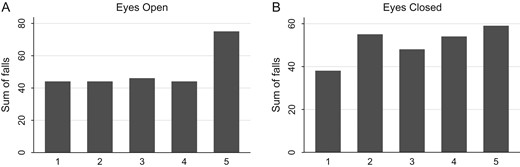
Distribution of falls over quintiles of postural sway length. Sway quintile classification for the EO (A) trial: Q1 = 161–249 mm, Q2 = 250–287 mm, Q3 = 288–333 mm, Q4 = 334–401 mm, Q5 ≥ 402 mm. Sway quintile classification for the EC (B) trial: Q1 = 211–461 mm, Q2 = 462–573 mm, Q3 = 574–699 mm, Q4 = 700–917 mm, Q5 ≥ 918 mm.
Postural sway parameters as independent predictors of incident falls
In the unadjusted model for EO trial data, the odds of falling were increased by 90% in the 5th postural sway quintile compared with the first (reference) quintile (odds ratio [OR] 1.90, 95% confidence interval [CI] 1.27–2.84; Table 2). In the second, fully adjusted model, the odds of falling were increased by 75% in the fifth quintile (OR 1.75, 95% CI 1.09–2.79). In this model, the odds of falling were also increased by 9% per 1-s increase in TUG test time (OR 1.09, 95% CI 1.03–1.16). Conversely, greater grip strength decreased the risk of falling, by 2% per 1-unit increase (OR 0.98, 95% CI 0.95–1.00).
Results of logistic regression models investigating postural sway parameters as independent predictors of incident falls
| Quintile | Model 1 (unadjusted) | Model 2 |
|---|---|---|
| OR (95% CI) | OR (95% CI) | |
| EO | ||
| 1 (ref) | – | – |
| 2 | 1.05 (0.67–1.64) | 0.91 (0.55–1.50) |
| 3 | 1.09 (0.70–1.69) | 1.05 (0.65–1.70) |
| 4 | 1.03 (0.66–1.61) | 1.05 (0.64–1.71) |
| 5 | 1.90 (1.27–2.84) | 1.75 (1.09–2.79) |
| EC | ||
| 1 (ref) | – | – |
| 2 | 1.51 (0.97–2.35) | 1.71 (1.05–2.81) |
| 3 | 1.24 (0.79–1.95) | 1.35 (0.80–2.26) |
| 4 | 1.46 (0.94–2.27) | 1.57 (0.95–2.61) |
| 5 | 1.65 (1.07–2.55) | 1.90 (1.12–3.22) |
| Quintile | Model 1 (unadjusted) | Model 2 |
|---|---|---|
| OR (95% CI) | OR (95% CI) | |
| EO | ||
| 1 (ref) | – | – |
| 2 | 1.05 (0.67–1.64) | 0.91 (0.55–1.50) |
| 3 | 1.09 (0.70–1.69) | 1.05 (0.65–1.70) |
| 4 | 1.03 (0.66–1.61) | 1.05 (0.64–1.71) |
| 5 | 1.90 (1.27–2.84) | 1.75 (1.09–2.79) |
| EC | ||
| 1 (ref) | – | – |
| 2 | 1.51 (0.97–2.35) | 1.71 (1.05–2.81) |
| 3 | 1.24 (0.79–1.95) | 1.35 (0.80–2.26) |
| 4 | 1.46 (0.94–2.27) | 1.57 (0.95–2.61) |
| 5 | 1.65 (1.07–2.55) | 1.90 (1.12–3.22) |
Model 1 investigated postural sway parameters and incident falls only. Model 2 further included sex, weight, histories of falls, smoking and CVD, MMSE score, total PA per day, grip strength and TUG test performance. Bold font indicates statistical significance (P < 0.05).
Results of logistic regression models investigating postural sway parameters as independent predictors of incident falls
| Quintile | Model 1 (unadjusted) | Model 2 |
|---|---|---|
| OR (95% CI) | OR (95% CI) | |
| EO | ||
| 1 (ref) | – | – |
| 2 | 1.05 (0.67–1.64) | 0.91 (0.55–1.50) |
| 3 | 1.09 (0.70–1.69) | 1.05 (0.65–1.70) |
| 4 | 1.03 (0.66–1.61) | 1.05 (0.64–1.71) |
| 5 | 1.90 (1.27–2.84) | 1.75 (1.09–2.79) |
| EC | ||
| 1 (ref) | – | – |
| 2 | 1.51 (0.97–2.35) | 1.71 (1.05–2.81) |
| 3 | 1.24 (0.79–1.95) | 1.35 (0.80–2.26) |
| 4 | 1.46 (0.94–2.27) | 1.57 (0.95–2.61) |
| 5 | 1.65 (1.07–2.55) | 1.90 (1.12–3.22) |
| Quintile | Model 1 (unadjusted) | Model 2 |
|---|---|---|
| OR (95% CI) | OR (95% CI) | |
| EO | ||
| 1 (ref) | – | – |
| 2 | 1.05 (0.67–1.64) | 0.91 (0.55–1.50) |
| 3 | 1.09 (0.70–1.69) | 1.05 (0.65–1.70) |
| 4 | 1.03 (0.66–1.61) | 1.05 (0.64–1.71) |
| 5 | 1.90 (1.27–2.84) | 1.75 (1.09–2.79) |
| EC | ||
| 1 (ref) | – | – |
| 2 | 1.51 (0.97–2.35) | 1.71 (1.05–2.81) |
| 3 | 1.24 (0.79–1.95) | 1.35 (0.80–2.26) |
| 4 | 1.46 (0.94–2.27) | 1.57 (0.95–2.61) |
| 5 | 1.65 (1.07–2.55) | 1.90 (1.12–3.22) |
Model 1 investigated postural sway parameters and incident falls only. Model 2 further included sex, weight, histories of falls, smoking and CVD, MMSE score, total PA per day, grip strength and TUG test performance. Bold font indicates statistical significance (P < 0.05).
In the unadjusted model used to examine EC trial data, the odds of falling were 65% higher in the 5th postural sway quintile than in the first quintile (OR 1.65, 95% CI 1.07–2.55). The fully adjusted model for EC trial data indicated that the odds of falling were 71% higher in the second quintile (OR 1.71, 95% CI 1.05–2.81) and 90% higher in the fifth quintile (OR 1.90, 95% CI 1.12–3.22; Table 2). In the EC trial model, TUG test performance and grip strength predicted incident falls in a similar manner as in the EO trial (data not shown).
Sensitivity analyses
Repeated WBB measures of total COP sway length revealed moderate test-retest reliability during EO trials (ICC3,1 = 0.60) and excellent reliability during EC trials (ICC3,1 = 0.94). WBB and BBS data showed a borderline moderate association for EO trials (r = 0.30, P = 0.002) and a strong association for EC trials (r = 0.77, P < 0.001). See Supplementary data, Appendix 1, available at Age and Ageing online.
Discussion
This study revealed that postural sway during quiet stance independently predicted incident falls after adjustment for multiple confounders, such as objective PA, functional mobility, presence of CVD and cognitive function, in a large cohort of 70-year-old men and women. Compared with the first quintile, the odds of falling were increased by 75–90% among participants in the fifth quintile of COP sway length (≥400 mm for the EO trial, ≥920 mm for the EC trial).
Several findings of the present study are novel and elaborate on previous findings regarding postural stability and falls. First, we detected a nonlinear distribution of falls over quintiles of COP sway length for the EO trial, with a markedly greater frequency of falls in the fifth quintile. This nonlinearity conveys potentially important information about the characteristics of falls, which might remain concealed when foregoing descriptive analyses or examining a small number of participants. Second, this study provides a basis for the investigation of certain cutoff values in relation to postural sway in older individuals, which could contribute to improved fall risk assessment by clinicians. Third, postural sway measured by the WBB proved to be an independent predictor of incident falls, even after multiple adjustments. This finding indicates that the objective static balance test is viable for fall risk assessment, although falls commonly occur during body movement and weight shifting [5].
We detected comparable ORs for incident falls in the highest quintiles of postural sway in both trials. Similar findings have been reported for measurements of sway under normal-vision and no-vision conditions [7]. However, the disparity in fall distribution between the EO and EC trials in this study suggests the existence of different underlying fall mechanisms. Further research is required to elucidate these findings and determine the potential consequences for fall risk assessment. One could argue that the measurement of postural sway and fall risk during an EO trial is plausible in relation to everyday fall circumstances, as participants likely maintain EO status. Impaired postural stability during EC trials, however, may be related to the occurrence of multiple falls [20], and many falls occur indoors during the evening and night due to darkness and limited vision [21].
This study is one of the largest to objectively investigate postural sway and prospective falls. Comparable studies have used retrospective fall data [9, 22] or included fewer participants with larger age ranges [23]. More importantly, although previous studies have reported conflicting results [8], we confirmed that the measurement of postural sway using a force platform is of value when identifying individuals at future risk of falling. Force platform measurement of postural stability provides objective and quantifiable data, which constitutes an advantage over clinical tests [12]. Furthermore, the WBB platform used in this study showed moderate to excellent test-retest reliability, supporting its utility for the measurement of postural stability. WBB data have also been shown to complement the prediction of prospective falls [14]. It is, however, important to recognise that clinical tests of balance are less expensive, as compared to force platform measurements. It would also be of interest to evaluate objective measures of postural sway against the fall risk assessment tool [24], which holistically approaches risk of falls.
Falls have multifactorial causes and involve factors such as mobility limitations, cognitive impairment, muscular weakness and CVD prevalence [4, 25, 26]. Fall-related risk factors such as previous falls, TUG test performance, MMSE score, grip strength and disease history were investigated in this study; none of them markedly influenced the relationship between increased postural sway and incident falls. Interestingly, TUG test performance also independently predicted falls by approximately 10% per 1-s increase in test time, results that are supported by a comparable cohort study [27].
This study has some limitations. First, we followed up on incident falls every 6 months, which may have led to difficulties in fall recollection for some participants. The fall rate of 14% is comparable to those reported in studies with similar fall recall designs [28, 29] and lower than reported with the use of shorter follow-up periods [23]. Nevertheless, fallers could be differentiated from non-fallers based on postural sway in this study, a finding supported by previous studies [7, 30]. Second, the observational study design prevented us from determining cause-effect relationships between falls and postural sway parameters. However, we followed up on falls prospectively, a clear advantage over the use of retrospective data when investigating the predictive ability of balance-measuring instruments. Third, we did not collect data on medication use, musculoskeletal conditions or neurological deficits, which are potential confounding factors and would have been of interest with respect to balance and falls. Finally, we included only participants aged 70 years, resulting in limited generalisability to fallers in other age groups, such as ‘healthy’ fallers at age 60–65, or ‘frail’ fallers at age 80–85. Although, data were automatically age adjusted, which is a study strength. Further strengths involve the large cohort studied and rich set of covariates examined, including objective measures of PA.
We conclude that objective measures of postural sway during quiet stance prospectively predict fall risk in 70-year-olds. This risk was increased by 75–90% for fallers compared with non-fallers in the highest quintile of COP sway length. In future studies, it would be valuable to examine the clinical utility of the investigated parameters in comparison to established clinical balance tests, and to investigate whether strategies to improve balance would reduce the fall risk.
This study measured postural sway objectively in almost 1900 participants, data on falls were collected prospectively.
Measures of postural sway independently predicted incident falls after multiple adjustments.
There was a nonlinear relationship between falls and postural sway during normal vision.
Postural sway over 400 mm during normal vision and over 920 mm during no vision increased the risk of falls by 75–90%.
Supplementary data
Supplementary data are available at Age and Ageing online.
Acknowledgements
The authors would like to thank Healthy Ageing Initiative research personnel Magnus Lindblom, David Lapveteläinen, and Jim Viklund, who were responsible for data collection.
Conflicts of interest
None declared.
Funding
This study was funded by the Swedish Research Council [grant number 2011-2976].

{kind=link}
Comments