




Why was the cohort set up?
Adolescence is the phase of life stretching between childhood and adulthood, for which a definition of 10–24 years has been recently proposed.1 Adolescence is a critical phase in life when an individual acquires the physical, cognitive, emotional, social and economic resources that are the foundation for health and well-being in later life.2 With regard to physical change, adolescence is characterized by dynamic brain development and drastic physical change owing to puberty.3,4 Especially, gradual maturation of prefrontal cortical function during adolescence enables higher-order mental processes including self-regulation.5 Humans can use this ability to regulate their own mind, and consciously and recursively develop themselves.
Other than dramatic physical change, environmental factors contribute to the social construct of adolescence as a distinct period of life, including the rise in education and social media exposure.6 Historically, since the pubertal timing has moved ahead but social role expectancy for adulthood has moved backward in recent years, mismatch of physical and mental maturity may likely occur in adolescence in the present day.7 The mismatch and an inappropriate maturation of self-regulation in adolescence could lead to the increased incidence of mental health problems among adolescents in modern society.8
Among health problems during adolescence, mental and substance use disorders are the leading cause of years lived with disability (YLDs),9 and approximately three-quarters of people with mental disorders have their onset before the age of 18.10 Further, in many countries including Japan, suicide is one of the leading causes of death in young people in recent years.11 Since brain change occurs during adolescence including the areas related to cognition, self-regulation and judgement,7 it may be reasonable to speculate that inappropriate brain maturation could lead to the emergence of mental disorders.5 Such brain and physical development occurs associated with both biological (genetics, epigenetics, natural endowments) and environmental (national and local policies, as well as community, school, workplace, peers, neighbourhood and family influences) factors. Thus, a life course approach with a multidisciplinary viewpoint is required to understand adolescent trajectories.6
Despite the importance of adolescence in the life course, few cohort studies have examined adolescent development using a prospective design. Physiological and psychological developmental processes during adolescence, factors affecting the process and interaction between them have not been sufficiently revealed. Our study, the Tokyo Teen Cohort study (TTC), is a prospective population-based birth cohort study aimed at investigating physiological and psychological development, including self-regulation, during adolescence. This multidisciplinary study collects data from various sources (parent, child, interviewer) via multiple methods (maternity record, self-report, interview, neurocognitive tests, biological measures and neuroimaging). Along with this main cohort study, a subsample study focusing on neuroimaging was also launched. The subsample study (population neuroscience TTC: pn-TTC) has conducted brain magnetic resonance imaging of children longitudinally and investigated the neurodevelopment of general adolescents. Given the focus of our project, early adolescence was an appropriate timing for the baseline survey.
Who is in the cohort?
TTC is a multidisciplinary longitudinal cohort study. The study is conducted at three municipalities in metropolitan area of Tokyo, Japan. The sample was recruited from the participants in the Tokyo Early Adolescence Survey (T-EAS),12 which was a cross-sectional survey on psychological and physical development of general adolescents 10 years old, and data from T-EAS were treated as the first wave of data for the TTC. Participants of T-EAS were recruited between October 2012 and January 2015. A broad range of adolescents from a wide geographical area, extending 9598 m2 in three municipalities (Setagaya-ku, Mitaka-shi, Chofu-shi) in the metropolitan area of Tokyo, were recruited into T-EAS (Figure 1). Children who lived in the municipalities and were born between September 2002 and August 2004 were recruited from the area using the resident register in each municipality. Among 18 830 eligible children, 14 553 children were randomly chosen due to a limited research budget (Figure 2). An invitation letter to T-EAS was sent approximately when participants turned 10 years old, and a trained interviewer visited their home after the letter was sent. The child’s primary parent (usually mother) gave written informed consent. Of 14 553 children, 4319 children could not be contacted. Of the 10 234 children who were accessible, 4478 children agreed to participate in T-EAS (response rate: 43.8%). The female ratio was lower in responders compared with non-responders (46.9% vs 49.8%, ϕ=0.03, p <0.01), and responders were less likely to be resident in Setagaya-ku and more likely to live in Mitaka-shi (Setagaya-ku: 62.6% vs 68.3%, Mitaka-shi: 18.3% vs 12.7%, V = 0.08, p <0.01), but there was no difference in birth month between participants and non-participants in T-EAS.
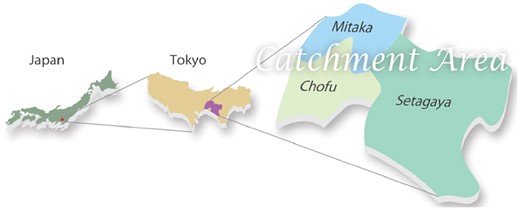
Catchment area of TTC.
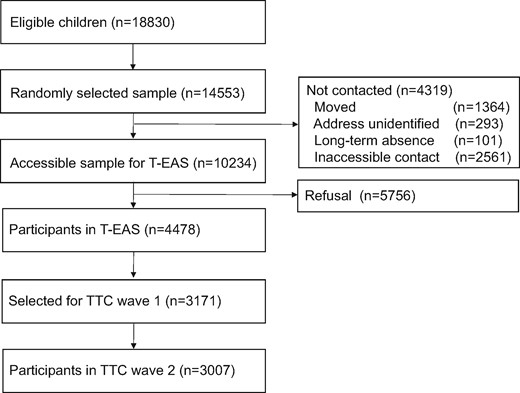
Flowchart of participant recruitment in TTC.
Candidate participants of TTC were chosen from 4478 children who participated in T-EAS. A total of 3000 children was the target number of participants in the second wave of TTC. When choosing the participants of TTC, no inclusion criteria were applied, but an oversampling method was used considering low follow-up rate of families with low annual household income. Among children who participated in T-EAS and had interest in participating in the cohort study, all 620 children whose household annual income was lower than 4990 thousand yen were invited. From the rest of 3858 children, 2551 children were randomly invited to the second wave of TTC. Demographic characteristics of the participants of TTC are shown in Table 1.
Demographic characteristics of participants in TTC (N = 3171)
| Number/mean | %/SD | |
|---|---|---|
| Sex | ||
| Female | 1487 | 53.1% |
| Male | 1684 | 46.9% |
| Age (months) | 122.10 | 3.30 |
| Mother’s country of origin (Japan) | 3117 | 98.3% |
| Father’s country of origin (Japan) | 2978 | 93.9% |
| Region | ||
| Setagaya | 1999 | 63.0% |
| Mitaka | 574 | 18.1% |
| Chofu | 598 | 18.9% |
| Single parent | 160 | 5.0% |
| Educational level of mother | ||
| High school or less | 524 | 16.5% |
| 2-year college | 1391 | 43.9% |
| 4-year university | 1126 | 35.5% |
| Graduate university | 105 | 3.3% |
| Educational level of father | ||
| High school or less | 542 | 17.1% |
| 2-year college | 409 | 12.9% |
| 4-year university | 1692 | 53.4% |
| Graduate university | 374 | 11.8% |
| Annual household income 10 000 yen) | ||
| 0-299 | 142 | 4.5% |
| 300-599 | 763 | 24.1% |
| 600-999 | 1224 | 38.6% |
| 1000+ | 917 | 28.9% |
| Number of siblings | 1.14 | 0.79 |
| Number of people in household | 4.20 | 0.95 |
| Number/mean | %/SD | |
|---|---|---|
| Sex | ||
| Female | 1487 | 53.1% |
| Male | 1684 | 46.9% |
| Age (months) | 122.10 | 3.30 |
| Mother’s country of origin (Japan) | 3117 | 98.3% |
| Father’s country of origin (Japan) | 2978 | 93.9% |
| Region | ||
| Setagaya | 1999 | 63.0% |
| Mitaka | 574 | 18.1% |
| Chofu | 598 | 18.9% |
| Single parent | 160 | 5.0% |
| Educational level of mother | ||
| High school or less | 524 | 16.5% |
| 2-year college | 1391 | 43.9% |
| 4-year university | 1126 | 35.5% |
| Graduate university | 105 | 3.3% |
| Educational level of father | ||
| High school or less | 542 | 17.1% |
| 2-year college | 409 | 12.9% |
| 4-year university | 1692 | 53.4% |
| Graduate university | 374 | 11.8% |
| Annual household income 10 000 yen) | ||
| 0-299 | 142 | 4.5% |
| 300-599 | 763 | 24.1% |
| 600-999 | 1224 | 38.6% |
| 1000+ | 917 | 28.9% |
| Number of siblings | 1.14 | 0.79 |
| Number of people in household | 4.20 | 0.95 |
Demographic characteristics of participants in TTC (N = 3171)
| Number/mean | %/SD | |
|---|---|---|
| Sex | ||
| Female | 1487 | 53.1% |
| Male | 1684 | 46.9% |
| Age (months) | 122.10 | 3.30 |
| Mother’s country of origin (Japan) | 3117 | 98.3% |
| Father’s country of origin (Japan) | 2978 | 93.9% |
| Region | ||
| Setagaya | 1999 | 63.0% |
| Mitaka | 574 | 18.1% |
| Chofu | 598 | 18.9% |
| Single parent | 160 | 5.0% |
| Educational level of mother | ||
| High school or less | 524 | 16.5% |
| 2-year college | 1391 | 43.9% |
| 4-year university | 1126 | 35.5% |
| Graduate university | 105 | 3.3% |
| Educational level of father | ||
| High school or less | 542 | 17.1% |
| 2-year college | 409 | 12.9% |
| 4-year university | 1692 | 53.4% |
| Graduate university | 374 | 11.8% |
| Annual household income 10 000 yen) | ||
| 0-299 | 142 | 4.5% |
| 300-599 | 763 | 24.1% |
| 600-999 | 1224 | 38.6% |
| 1000+ | 917 | 28.9% |
| Number of siblings | 1.14 | 0.79 |
| Number of people in household | 4.20 | 0.95 |
| Number/mean | %/SD | |
|---|---|---|
| Sex | ||
| Female | 1487 | 53.1% |
| Male | 1684 | 46.9% |
| Age (months) | 122.10 | 3.30 |
| Mother’s country of origin (Japan) | 3117 | 98.3% |
| Father’s country of origin (Japan) | 2978 | 93.9% |
| Region | ||
| Setagaya | 1999 | 63.0% |
| Mitaka | 574 | 18.1% |
| Chofu | 598 | 18.9% |
| Single parent | 160 | 5.0% |
| Educational level of mother | ||
| High school or less | 524 | 16.5% |
| 2-year college | 1391 | 43.9% |
| 4-year university | 1126 | 35.5% |
| Graduate university | 105 | 3.3% |
| Educational level of father | ||
| High school or less | 542 | 17.1% |
| 2-year college | 409 | 12.9% |
| 4-year university | 1692 | 53.4% |
| Graduate university | 374 | 11.8% |
| Annual household income 10 000 yen) | ||
| 0-299 | 142 | 4.5% |
| 300-599 | 763 | 24.1% |
| 600-999 | 1224 | 38.6% |
| 1000+ | 917 | 28.9% |
| Number of siblings | 1.14 | 0.79 |
| Number of people in household | 4.20 | 0.95 |
TTC is based at three research institutes: Tokyo Metropolitan Institute of Medical Science, the University of Tokyo and SOKENDAI (Graduate University for Advanced Studies). Ethics approval has been granted by all of the three institutions.
How often have they been followed up?
Data collection every 2 years is currently planned. The first wave of data collection took place between 2012 and 2015, and the second wave took place between 2014 and 2017. The third wave of data collection has started from March 2017 and is currently being conducted. Of the 3171 children who were invited, 3007 individuals participated in the second wave of TTC (follow-up rate 94.8%). When comparing those who were followed up and who were lost to follow-up, there were no differences in demographic characteristics including age (mean 122.1 months vs 122.0 months, p = 0.61), sex (female ratio 47.2% vs 42.1%, p = 0.20), number of siblings (mean 1.14 vs 1.12, p = 0.80), paternal education (mean 4.60 vs 4.62, p = 0.79) or maternal education (mean 4.25 vs 4.20, p = 0.51). In wave 1, a self-report questionnaire was administered and physical examination and interview at home were conducted with both children and parents by the interviewers. A similar method was applied to collect data by the interviewers in wave 2. In addition, a touch-panel device (iPad, Apple Inc., USA) was used to measure some aspects of cognitive function of children and parents in wave 2. In wave 3, similar to wave 1, both self-report questionnaire and interview were used to collect data. Along with TTC, the subsample study pn-TTC has also been conducted. The details of the pn-TTC are described elsewhere.13
Sample maintenance
To maintain the attrition rate low, we have actively sought to retain the interest and compliance of the young sample in our cohort. We maintain contact with participating families via customized birthday cards, a semi-annual newsletter, ‘change of address’ postcards and ‘thank you’ cards for the participants. Parents were asked to provide contact details that will be used for tracing participants at future waves if necessary. The TTC website [http://ttcp.umin.jp/], on which we post commentaries, research members and selected observations, will serve as a repository for reporting findings.
What has been measured?
Table 2 presents a summary of measures and the waves at which they were collected. This paper describes wave 1 in detail, noting any changes in later waves. Data were collected at home from the child and a primary parent (usually mother) by both interview and self-report questionnaires. There were two sets of questionnaires (part 1 and part 2) for both child and a parent. Trained interviewers visited the participant’s home twice to collect data. Many children had the same interviewer for each of the waves, but some children had different interviewers for the series of waves. For example, 63.1% of children had the same interviewer for wave 1 and wave 2. At the first visit, written informed consent was obtained and part 1 self-report questionnaires were distributed to child and a parent. The questionnaire usually takes about approximately 25 to 35 min for children and 20 to 40 min for parents to complete. Then, at the second visit, anthropometric measurement was completed for child, and part 2 self-report questionnaires were distributed to child and a parent. The part 2 questionnaire was distributed along with an envelope to seal it in when completed, in order for participants to be able to answer without being seen by other family members. Those were collected by the interviewers immediately after completion. Further, an interviewer conducted a structured interview for both the child and a parent. The structured interview was conducted for child and parent separately, and they were not present for each other’s interview. The interview for the child included cognitive tests. Further, an interviewer answered a short questionnaire on the child’s character/behaviours after home visits were completed. In wave 2, iPad application was used to administer cognitive tests, and saliva and urine samples were collected after interview.
Measures and time points in TTC
| Method | Construct | Measures | Source | Wave (age of participants in years) | ||
|---|---|---|---|---|---|---|
| 1 (10 years) | 2 (12 yreas) | 3 (14 years) | ||||
| Self-report questionnaire | Mental health and behaviour problems | Self-organization | Interviewer | ✓ | ✓ | |
| SDQ, CBCL | Parent | ✓ | ✓ | ✓ | ||
| TIC | Parent | ✓ | ✓ | |||
| SMFQ, APSS | Child | ✓ | ✓ | ✓ | ||
| Psychological well-being | WHO-5 | Child | ✓ | ✓ | ✓ | |
| Psychological development, Character | CNSIE, MCQ, CPAQ, sensation-seeking | Child | ✓ | ✓ | ||
| Personalized values, aspirations | Parent/child | ✓ | ✓ | ✓ | ||
| Personal relationships | Bullying, help-seeking, romantic relationship, family relationship | Parent/child | ✓ | ✓ | ✓ | |
| Academic achievement | Performance in school | Parent | ✓ | ✓ | ✓ | |
| Physical health, nutrition and other problems | Special health care needs, medication, sleep habit | Parent | ✓ | ✓ | ✓ | |
| Extracurricular activity | Parent/child | ✓ | ✓ | ✓ | ||
| Internet addiction | Parent | ✓ | ✓ | ✓ | ||
| Cellphone use, TV viewing | Parent | ✓ | ✓ | |||
| Pubertal development | Tanner stage, physical change | Parent/child | ✓ | ✓ | ✓ | |
| Life event | Separation from parents, bereavement | Parent | ✓ | ✓ | ✓ | |
| Environment | School environment, private school use, neighbourhood | Parent/child | ✓ | ✓ | ✓ | |
| Parenting | Style of parenting | ✓ | ✓ | ✓ | ||
| Parent health | Medication, smoking, alcohol use | Parent | ✓ | ✓ | ✓ | |
| Parental mental health | K6, GHQ, purpose in life | Parent | ✓ | ✓ | ✓ | |
| Parental cognitive function | JART | Parent | ✓ | |||
| Social support for parent, demographics | SSQ, family composition, parental age, national origin, education, work, annual household income | Parent | ✓ | ✓ | ✓ | |
| Maternity record | Prenatal and postnatal factors | Gestational age, medical condition during pregnancy, smoking, alcohol use, mode of delivery, anthropometry at birth | Maternity record | ✓ | ||
| Breastfeeding | Maternity record | ✓ | ||||
| Anthropometry during infancy | Maternity record | ✓ | ||||
| Developmental milestones | Maternity record | ✓ | ||||
| Nursery use | Parent | ✓ | ||||
| Anthropometric measurement | Anthropometry | Height, weight, grip | Interviewer | ✓ | ✓ | ✓ |
| Length of finger | Interviewer | ✓ | ||||
| Interview | Cognitive function | WISC-III | Interviewer | ✓ | ✓ | |
| iPad | Inhibition, risk taking | Go No-go task, BART | iPad | ✓ | ||
| Saliva sampling | DNA, hormones etc. | DNA, hormone etc. | Child | ✓ | ||
| Urine sampling | Trace element etc. | Trace element etc. | Child | ✓ | ✓ | |
| Method | Construct | Measures | Source | Wave (age of participants in years) | ||
|---|---|---|---|---|---|---|
| 1 (10 years) | 2 (12 yreas) | 3 (14 years) | ||||
| Self-report questionnaire | Mental health and behaviour problems | Self-organization | Interviewer | ✓ | ✓ | |
| SDQ, CBCL | Parent | ✓ | ✓ | ✓ | ||
| TIC | Parent | ✓ | ✓ | |||
| SMFQ, APSS | Child | ✓ | ✓ | ✓ | ||
| Psychological well-being | WHO-5 | Child | ✓ | ✓ | ✓ | |
| Psychological development, Character | CNSIE, MCQ, CPAQ, sensation-seeking | Child | ✓ | ✓ | ||
| Personalized values, aspirations | Parent/child | ✓ | ✓ | ✓ | ||
| Personal relationships | Bullying, help-seeking, romantic relationship, family relationship | Parent/child | ✓ | ✓ | ✓ | |
| Academic achievement | Performance in school | Parent | ✓ | ✓ | ✓ | |
| Physical health, nutrition and other problems | Special health care needs, medication, sleep habit | Parent | ✓ | ✓ | ✓ | |
| Extracurricular activity | Parent/child | ✓ | ✓ | ✓ | ||
| Internet addiction | Parent | ✓ | ✓ | ✓ | ||
| Cellphone use, TV viewing | Parent | ✓ | ✓ | |||
| Pubertal development | Tanner stage, physical change | Parent/child | ✓ | ✓ | ✓ | |
| Life event | Separation from parents, bereavement | Parent | ✓ | ✓ | ✓ | |
| Environment | School environment, private school use, neighbourhood | Parent/child | ✓ | ✓ | ✓ | |
| Parenting | Style of parenting | ✓ | ✓ | ✓ | ||
| Parent health | Medication, smoking, alcohol use | Parent | ✓ | ✓ | ✓ | |
| Parental mental health | K6, GHQ, purpose in life | Parent | ✓ | ✓ | ✓ | |
| Parental cognitive function | JART | Parent | ✓ | |||
| Social support for parent, demographics | SSQ, family composition, parental age, national origin, education, work, annual household income | Parent | ✓ | ✓ | ✓ | |
| Maternity record | Prenatal and postnatal factors | Gestational age, medical condition during pregnancy, smoking, alcohol use, mode of delivery, anthropometry at birth | Maternity record | ✓ | ||
| Breastfeeding | Maternity record | ✓ | ||||
| Anthropometry during infancy | Maternity record | ✓ | ||||
| Developmental milestones | Maternity record | ✓ | ||||
| Nursery use | Parent | ✓ | ||||
| Anthropometric measurement | Anthropometry | Height, weight, grip | Interviewer | ✓ | ✓ | ✓ |
| Length of finger | Interviewer | ✓ | ||||
| Interview | Cognitive function | WISC-III | Interviewer | ✓ | ✓ | |
| iPad | Inhibition, risk taking | Go No-go task, BART | iPad | ✓ | ||
| Saliva sampling | DNA, hormones etc. | DNA, hormone etc. | Child | ✓ | ||
| Urine sampling | Trace element etc. | Trace element etc. | Child | ✓ | ✓ | |
Measures and time points in TTC
| Method | Construct | Measures | Source | Wave (age of participants in years) | ||
|---|---|---|---|---|---|---|
| 1 (10 years) | 2 (12 yreas) | 3 (14 years) | ||||
| Self-report questionnaire | Mental health and behaviour problems | Self-organization | Interviewer | ✓ | ✓ | |
| SDQ, CBCL | Parent | ✓ | ✓ | ✓ | ||
| TIC | Parent | ✓ | ✓ | |||
| SMFQ, APSS | Child | ✓ | ✓ | ✓ | ||
| Psychological well-being | WHO-5 | Child | ✓ | ✓ | ✓ | |
| Psychological development, Character | CNSIE, MCQ, CPAQ, sensation-seeking | Child | ✓ | ✓ | ||
| Personalized values, aspirations | Parent/child | ✓ | ✓ | ✓ | ||
| Personal relationships | Bullying, help-seeking, romantic relationship, family relationship | Parent/child | ✓ | ✓ | ✓ | |
| Academic achievement | Performance in school | Parent | ✓ | ✓ | ✓ | |
| Physical health, nutrition and other problems | Special health care needs, medication, sleep habit | Parent | ✓ | ✓ | ✓ | |
| Extracurricular activity | Parent/child | ✓ | ✓ | ✓ | ||
| Internet addiction | Parent | ✓ | ✓ | ✓ | ||
| Cellphone use, TV viewing | Parent | ✓ | ✓ | |||
| Pubertal development | Tanner stage, physical change | Parent/child | ✓ | ✓ | ✓ | |
| Life event | Separation from parents, bereavement | Parent | ✓ | ✓ | ✓ | |
| Environment | School environment, private school use, neighbourhood | Parent/child | ✓ | ✓ | ✓ | |
| Parenting | Style of parenting | ✓ | ✓ | ✓ | ||
| Parent health | Medication, smoking, alcohol use | Parent | ✓ | ✓ | ✓ | |
| Parental mental health | K6, GHQ, purpose in life | Parent | ✓ | ✓ | ✓ | |
| Parental cognitive function | JART | Parent | ✓ | |||
| Social support for parent, demographics | SSQ, family composition, parental age, national origin, education, work, annual household income | Parent | ✓ | ✓ | ✓ | |
| Maternity record | Prenatal and postnatal factors | Gestational age, medical condition during pregnancy, smoking, alcohol use, mode of delivery, anthropometry at birth | Maternity record | ✓ | ||
| Breastfeeding | Maternity record | ✓ | ||||
| Anthropometry during infancy | Maternity record | ✓ | ||||
| Developmental milestones | Maternity record | ✓ | ||||
| Nursery use | Parent | ✓ | ||||
| Anthropometric measurement | Anthropometry | Height, weight, grip | Interviewer | ✓ | ✓ | ✓ |
| Length of finger | Interviewer | ✓ | ||||
| Interview | Cognitive function | WISC-III | Interviewer | ✓ | ✓ | |
| iPad | Inhibition, risk taking | Go No-go task, BART | iPad | ✓ | ||
| Saliva sampling | DNA, hormones etc. | DNA, hormone etc. | Child | ✓ | ||
| Urine sampling | Trace element etc. | Trace element etc. | Child | ✓ | ✓ | |
| Method | Construct | Measures | Source | Wave (age of participants in years) | ||
|---|---|---|---|---|---|---|
| 1 (10 years) | 2 (12 yreas) | 3 (14 years) | ||||
| Self-report questionnaire | Mental health and behaviour problems | Self-organization | Interviewer | ✓ | ✓ | |
| SDQ, CBCL | Parent | ✓ | ✓ | ✓ | ||
| TIC | Parent | ✓ | ✓ | |||
| SMFQ, APSS | Child | ✓ | ✓ | ✓ | ||
| Psychological well-being | WHO-5 | Child | ✓ | ✓ | ✓ | |
| Psychological development, Character | CNSIE, MCQ, CPAQ, sensation-seeking | Child | ✓ | ✓ | ||
| Personalized values, aspirations | Parent/child | ✓ | ✓ | ✓ | ||
| Personal relationships | Bullying, help-seeking, romantic relationship, family relationship | Parent/child | ✓ | ✓ | ✓ | |
| Academic achievement | Performance in school | Parent | ✓ | ✓ | ✓ | |
| Physical health, nutrition and other problems | Special health care needs, medication, sleep habit | Parent | ✓ | ✓ | ✓ | |
| Extracurricular activity | Parent/child | ✓ | ✓ | ✓ | ||
| Internet addiction | Parent | ✓ | ✓ | ✓ | ||
| Cellphone use, TV viewing | Parent | ✓ | ✓ | |||
| Pubertal development | Tanner stage, physical change | Parent/child | ✓ | ✓ | ✓ | |
| Life event | Separation from parents, bereavement | Parent | ✓ | ✓ | ✓ | |
| Environment | School environment, private school use, neighbourhood | Parent/child | ✓ | ✓ | ✓ | |
| Parenting | Style of parenting | ✓ | ✓ | ✓ | ||
| Parent health | Medication, smoking, alcohol use | Parent | ✓ | ✓ | ✓ | |
| Parental mental health | K6, GHQ, purpose in life | Parent | ✓ | ✓ | ✓ | |
| Parental cognitive function | JART | Parent | ✓ | |||
| Social support for parent, demographics | SSQ, family composition, parental age, national origin, education, work, annual household income | Parent | ✓ | ✓ | ✓ | |
| Maternity record | Prenatal and postnatal factors | Gestational age, medical condition during pregnancy, smoking, alcohol use, mode of delivery, anthropometry at birth | Maternity record | ✓ | ||
| Breastfeeding | Maternity record | ✓ | ||||
| Anthropometry during infancy | Maternity record | ✓ | ||||
| Developmental milestones | Maternity record | ✓ | ||||
| Nursery use | Parent | ✓ | ||||
| Anthropometric measurement | Anthropometry | Height, weight, grip | Interviewer | ✓ | ✓ | ✓ |
| Length of finger | Interviewer | ✓ | ||||
| Interview | Cognitive function | WISC-III | Interviewer | ✓ | ✓ | |
| iPad | Inhibition, risk taking | Go No-go task, BART | iPad | ✓ | ||
| Saliva sampling | DNA, hormones etc. | DNA, hormone etc. | Child | ✓ | ||
| Urine sampling | Trace element etc. | Trace element etc. | Child | ✓ | ✓ | |
Children’s psychological development/health
Psychological development was evaluated from several aspects. Locus of control (the extent to which one perceives a causal connection between one’s behaviour or cognition and subsequent outcomes) was measured by the short form of the Children’s Nowicki-Strickland Internal-External Scale (CNSIE).14 In order to evaluate how children assessthe future consequences of their actions, a delay-discount rate was assessed using the Monetary Choice Questionnaire (MCQ).15 The Childhood Personality Attribute Questionnaire (CPAQ) was utsed to assess psychological masculinity and femininity.16 In addition, questions about sensation-seeking, empathy, attitude to helping others and sense of time were also asked.
Self-organization was one of the focuses of psychological development of the children. The assessment of self-organization was started after the initial 1500 interviews were completed. Children’s self-organization was assessed by interviewer comparing the child with other children they had seen. Four items were used for assessment including attitude to work, concentration, neatness in work and daydreaming during the home visit.17
Mental health and behavioural problems were also major focuses of this study. Those measurements included the Strength and Difficulties Questionnaire (SDQ),18 the Child Behavior Checklist (CBCL),19 the Short Mood and Feelings Questionnaire (SMFQ)20 and the Japanese version of the Adolescent Psychotic-Like Symptom Screener (APSS)21 which is composed of seven items selected from the Diagnostic Interview Schedule for Children (DISC),22 corresponding to psychotic symptoms including hallucination and delusion.23 Psychological well-being was measured by the WHO-Five Well-Being Index (WHO-5).24
In terms of personal relationships, bullying involvement was assessed using self-report questions according to the definition of bullying defined in the Olweus Bully/Victims Questionnaire (OBQ).25 In addition to the report from children, main carers were separately asked about bullying involvement of their children. Leadership, quarrels with friends, help-seeking for depression, and romantic relationship were also asked. Further, by asking both children and parents, we assessed family relationships including conversation, weekends and help with homework.
Since individuals’ hierarchies of values stabilize during adolescence,26 we assessed the personalized values and future aspirations of adolescents using free-writing questions and original questionnaires. Further, because the development of the individual’s values are affected by social and family environment,26,27 we also assessed the personalized values of primary parents and their aspirations for their children’s future, to examine the trans-generational shape of values and behaviours.
Children’s cognitive development
Two subtests (information, picture completion) were selected from the Wechsler Intelligence Scale for Children (WISC-III) to test cognitive function of children, referring to the short form of the WISC-III in the previous study.28 We gave full version of the WISC-III by expert psychologists to 28 children from T-EAS participants after 1 year from the initial survey. There was acceptable reliability of measurements of Intelligence and Picture Completion (Cronbach’s α = 0.70 and 0.54, respectively). Considering the result from the multiple regression analysis with full IQ as dependent variable and the two subtests as independent variables (adjusted R2 = 0.78), we developed a formula for estimating children’s IQ from the two subtests. In addition to the WISC-III, the Go No-go task29 and the Balloon Analogue Risk Test30 were conducted using iPad in wave 2. In addition, primary parents evaluated children’s academic performance at school using a five-point Likert scale for each academic subject. In Japan, all public elementary schools issue a report card for each student, evaluating achievement in each subject by the same standards in the absolute scale (‘Satisfactory’, ‘Almost satisfactory’, ‘More efforts needed’).
Children’s physical development/health
Height, weight, grip and length of forefinger and third finger of the child were measured at home by a specially trained interviewer. Pubertal development was evaluated by both a child and a primary parent. A primary parent assessed the children’s pubertal development by choosing pictures of bodies according to the Tanner stage (breast and pubertal hair for girls, and genital development and pubertal hair for boys).31,32 Apart from evaluation by a primary parent, children evaluated themselves on acne, pubertal hair, breast (female), menarche (female), voice breaking (male) and beard (male).
With regard to physical health, needs of special health care was also evaluated by a primary parent.33 In terms of life habit, appetite, sleep habit, dietary habit, extracurricular activities including music, painting, exercise and reading were asked. Further, addictive use of internet was assessed using questions used in the previous study.34
For the purpose of further biological investigation, in wave 2, saliva and urine samples were collected from all participants in TTC. Measurements including sex hormones and oxidative stress have been planned. In wave 3, urine samples were collected from all participants in TTC.
Further, we selected a subsample from TTC and conducted a prospective biological examination focusing on population neuroscience in a longitudinal design (pn-TTC). The examination includes neuroimaging using brain magnetic resonance imaging (MRI) as well as saliva sampling (DNA and gonadal and adrenal hormones). We recruited about 300 children into the subsample study. The subsample cohort study was initiated about 1 year after TTC, and has been carried out in parallel with TTC.
Perinatal environment
Perinatal information was gathered from the Maternal and Child Health handbook which is distributed to all pregnant mothers in Japan.35 Pregnant women in Japan bring the book to health check-ups during pregnancy and after childbirth. The recorded data included mother’s anthropometry, smoking, drinking during pregnancy, fetal growth, mode of delivery, breastfeeding, birthweight, growth in infancy and developmental milestones. Use of nursery and working status of parents during childhood were also assessed in the self-report questionnaire.
Household environment
Number of siblings in the household was asked in the interview of the primary parent conducted at a home visit. Marital status of parents, educational level of parents and annual household income were assessed by the self-report questionnaire. Information on the parent focused on physical and mental health of parents, which included parental psychological distress assessed by K6,36 and purpose in life.37 Parental cognitive function was evaluated using the 25-item Japanese version of the National Adult Reading Test (JART).38,39 Social support for the parent was assessed using a six-item instrument of the Social Support Questionnaire (SSQ6).40,41
What has been found so far? Key findings and publications
More than 10 manuscripts are currently submitted or in preparation for publication. A complete list of publications will be available on the TTC website [http://ttcp.umin.jp/publications.html]. Some of the findings from TTC relate to psychological mechanisms indicating the association between the children’s experiences and psychological health. One study examined the association between experience of being bullied, dissociation and hallucinatory experiences. This study suggested that dissociation was a mediator in the relation between peer victimization and hallucinatory experiences in early adolescence.12 Another study investigated the association between enuresis and behavioural problems of early adolescents. This study revealed that enuresis was independently associated with hyperactivity-inattention among the general population as measured by the Strength and Difficulties Questionnaire.42 Help-seeking intention was also a focus of TTC, and a study examined the factors and sex difference in help-seeking intention in early adolescents. The study revealed that girls had more help-seeking intention for depression than boys. Further, this study also investigated factors associated with help-seeking intention, and gender norms inhibited help-seeking intention more strongly in boys than in girls.43 Some of our studies focused on physical and psychological health of mothers of adolescents. A study examined the association between purpose in life and tobacco use of mothers, and revealed that greater purpose in life was associated with a decreased likelihood of tobacco use.44
What are the main strengths and weaknesses?
One of the main strengths of TTC is its prospective research design and the multidisciplinary nature of the data. The prospective design enables analyses of changes over time, and the multidisciplinary nature of the data enables more in-depth understanding of the physical and psychological development including self-regulation. Second, measurements uncommonly done in other large cohort studies, such as saliva and urine sampling, facilitates analysis of biological factors affecting physical and psychological development. Third, an international advisory board has also been established. The board consists of international experts in a multidisciplinary field of science including epidemiology, neuroscience and social science. There is a possibility of a cross-cohort study in the future in collaboration with the advisory board. Fourth, the follow-up rate is as high as 94.8% in the second wave. This high follow-up rate would enhance the generalizability of the results from our cohort study. Fifth, since most participants have the same ethnic origin, investigation of biological factors in the homogeneous group can be conducted.
The weaknesses of TTC include the timing of start of the cohort study. Since TTC started at 10 years age, some information on infancy and childhood may suffer from recall bias. However, because the Maternal and Child Health handbook is distributed to all pregnant mothers in Japan, this may substantially cover the limitation. Since the sample of TTC was recruited from a small number of metropolitan municipalities in Tokyo, social background of TTC participants may not fully represent all residents in Tokyo. In order to overcome this limitation, we have done oversampling of participants in a survey (T-EAS) to recruit samples of TTC. Since the participation rate in T-EAS (18 830 eligible children, 4478 participants = 23.8%) was low; there is a certain limitation about the representativeness of the study sample. Because most participants have the same ethnic origin, caution is needed when expanding the study results into other ethnic groups. Although we gave the same training for interviewers beforehand, we did not measure inter-rater variability for assessing self-organization of children.
Can I get hold of the data? Where can I find out more?
Data from TTC is archived in the Tokyo Metropolitan Institute of Medical Science. Collaboration in data analysis and publication will be welcome through specific research proposals sent to the research committee. The initial contact point for collaborations is [nishida-at@igakuken.or.jp].
TTC is a transgenerational prospective population-based birth cohort study aimed at investigating physiological and psychological development, including self-regulation and personalized values, during adolescence.
TTC was launched in 2012, and 3171 10-year-old children were recruited from 4478 children who participated in a cross-sectional survey (T-EAS). Of 10 234 children who lived in the three municipalities in Tokyo and were born between September 2002 and August 2004, 4478 children participated in T-EAS.
Follow-up has been conducted every 2 years. Data collection was conducted by self-report questionnaire and interview for both children and primary parent, and urine and saliva were also collected. Along with TTC, a subsample study focusing on neuroimaging (pn-TTC) has also been conducted.
The dataset comprises a wide range of multidisciplinary measurement including the biological, cognitive, psychological and physical development of children. Also, perinatal, family and school environments were measured.
Collaboration in data analysis and publication will be welcome through specific research proposals sent to the research committee. The initial contact point for collaborations is [nishida-at@igakuken.or.jp].
Funding
This work was supported by Grant-in-Aid for Scientific Research on Innovative Areas (23118002; Adolescent Mind & Self-Regulation) from the Ministry of Education, Culture, Sports, Science and Technology of Japan. This study was also supported by JSPS KAKENHI Grant Numbers JP16HY06395, 16H06398, 16H06399, 16K21720, 16K15566, and 17H05931. This work was supported in part by UTokyo Center for Integrative Science of Human Behavior (CiSHuB) and by the International Research Center for Neurointelligence (WPI-IRCN) at the University of Tokyo Institutes for Advanced Study (UTIAS).
Conflict of interest: None declared.
References
Author notes
Shuntaro Ando and Atsushi Nishida authors contributed equally to this work.


{kind=link}
{kind=link}